Neoplasia Colorettale
Farmaci anti VEGF-alfa, VEGFR e anti-EFGR nell’era del
mantenimento biologico post-progressione: basi molecolari,
razionale di utilizzo e necessità di studio
Andrea Mancuso, MD
Department of Medical Oncology,
San Camillo and Forlanini Hospitals, Rome, Italy
Scopo della Relazione - mCRC -
Comprendere da dove nascono le indicazioni biologiche del Bevacizumab
Comprendere le basi molecolari del Cetuximab e valutare la sua azione
come “mantenimento” di risposta e in assetto post progressione
Comprendere le basi molecolari di efficacia del Panitumumab, l’utilizzo
terapeutico e la sequenza biologica ideale
Comprendere la biologia molecolare dell’Aflibercept e implementare
possibili scenari futuri e nicchie di utilizzo
Possiamo fare di meglio?
Judah Folkman: Padre dell’Angiogenesi
• Prima persona ad osservare
l’angiogenesi come
meccanismo patogenetico nel
cancro già dal 1971
• Primo a stabilire correlazione
tra Microambiente e Tumore
• Primo a definire il concetto di
crescita
sostenuta
dal
microambiente perineoplastico
versus una crescita tumorale
totalmente indipendente
Mori et al. Blood Cancer Journal, 2012
Direct angiogenesis inhibitors prevent vascular endothelial
cells from proliferating or migrating toward the tumor.
Judah Folkman: Padre dell’Angiogenesi
• E’ possibile controllare la crescita di
tumori umani agendo sul
microambiente anziché direttamente
sulla cellula neoplastica
– Talidomide nel mieloma
– Bevacizumab nei tumori del colon
– Rituximab nel linfoma di Hodgkin
classico (CD20-neg)
– Terapia anti H. Pylori nel linfoma MALT
dello stomaco
– Prevenzione dei tumori del colon-retto
con farmaci anti-infiammatori
(NSAIDs)
Mori et al. Blood Cancer Journal, 2012
Bevacizumab
Recombinant, humanized monoclonal antibody that binds to all
isoforms of VEGF-A such that KDR signaling is inhibited
Ang-1
Endost.
Ang-2
PDGF
PIGF
MMP
TSP-1
IL-12
HGF
Angiost.
Tumstatin
sIL2R
bFGF
Platelect factor 4
Mori et al. Blood Cancer Journal, 2012
Bevacizumab
“The emergence of resistance depends in part on the genetic
instability, heterogeneity and high mutational rate of tumour cells.
In contrast, endothelial cells are genetically stable, homogenous
and have a low mutational rate”
“Therefore, anti-angiogenic therapy directed against a tumour’s
endothelial cells should, in principle, induce little or no drug
resistance”
Boehm et al. Nature, 1997
Bevacizumab
“An unexpected finding is that repeated cycles of antiangiogenic
therapy are followed by prolonged tumour dormancy”
“Antiangiogenic therapy needs to be maintained to prolong the
stability of the tumor and to have a reduced growth of disease in
the case of direct progression of the neoplastic cells”
Concetto di mantenimento e post-progressione (1997)
Boehm et al. Nature, 1997
Clinical hypothesis: observational studies of post-progression
bevacizumab – BRITE (AVF2941n) and ARIES (AVF3991n)
No post-PD
treatment
(n=282)
ARIES1
BRiTE2
Unresectable mCRC treated
with first-line bevacizumab +
chemotherapy (n=1,548)
Unresectable mCRC treated
with first-line bevacizumab +
chemotherapy (n=1,953)
First progression (n=1,026*)
First progression (n=1,445)
Physician decision
(no randomisation)
Physician decision
(no randomisation)
No
bevacizumab
post-PD
(n=336)
*Patients alive 2 months after PD
Bevacizumab
post-PD
(n=408)
No post-PD
treatment
(n=253)
No
bevacizumab
post-PD
(n=531)
CRC
Bevacizumab
post-PD
(n=642)
1. Cohn, et al. WCGC 2010; 2. Grothey, et al. JCO 2008
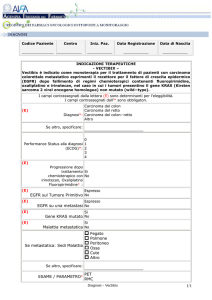
BRiTEa: Significantly improved OS with postprogression bevacizumab (BBP) therapy
CRC
1.0
BBP (n=642)
No BBP (n=531)
No treatment (n=253)
Estimated probability
0.8
0.6
0.4
12.6
HR=2.05
(95% CI 1.64–2.56)
p<0.001
0.2
0
0
5
10
19.9
15
20
31.8
HR=0.49
(95% CI 0.41–0.58)
p<0.001
25
30
35
OS (months)
Grothey ASCO 2007
Grothey JCO 2008
ARIES: Survival beyond progression according to
post-progression bevacizumab exposure
1.0
Survival beyond
progression
Median, months
HR (95% CI)
Estimated probability
0.8
CRC
No BBP
BBP
(n=336)
(n=408)
7.5
14.1
0.52 (0.42–0.63)
p<0.001
0.6
0.4
0.2
7.5
14.1
0
0
5
10
15
20
25
30
Survival beyond progression (months)
Cohn ASCO 2010
ML18147 study design (phase III)
BEV + standard
first-line CT (either
oxaliplatin or
irinotecan-based)
(n=820)
Standard second-line CT
(oxaliplatin or irinotecanbased) until PD
PD
Randomise 1:1
CT switch:
→ Irinotecan
Irinotecan→ Oxaliplatin
Oxaliplatin
BEV (2.5 mg/kg/wk) +
standard second-line CT
(oxaliplatin or irinotecanbased) until PD
Primary endpoint
• Overall survival (OS) from randomisation
Secondary endpoints
included
• Progression-free survival (PFS)
• Best overall response rate
• Safety
• First-line CT (oxaliplatin-based, irinotecan-based)
Stratification factors
• First-line PFS (≤9 months, >9 months)
• Time from last BEV dose (≤42 days, >42 days)
• ECOG PS at baseline (0/1, 2)
Study conducted in 220 centres in Europe and Saudi Arabia
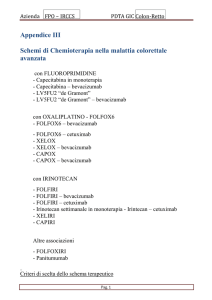
OS: ITT population
1.0
CT (n=410)
BEV + CT (n=409)
OS estimate
0.8
0.6
Unstratifieda HR: 0.81 (95% CI: 0.69–0.94)
p=0.0062 (log-rank test)
0.4
Stratifiedb HR: 0.83 (95% CI: 0.71–0.97)
p=0.0211 (log-rank test)
0.2
9.8 mo
0
0
6
11.2 mo
12
18
24
30
36
42
Time (months)
No. at risk
CT
410
293
162
51
24
7
3
2
0
BEV + CT 409
328
188
64
29
13
4
1
0
Median follow-up:
CT, 9.6 months (range 0–45.5); BEV + CT, 11.1 months (range 0.3–44.0)
aPrimary
analysis method; bStratified by first-line CT (oxaliplatin-based, irinotecan-based), first-line PFS (≤9 months, >9 months), time from last dose
of BEV (≤42 days, >42 days), ECOG performance status at baseline (0, ≥1)
48
Bevacizumab
Sulle basi molecolari fornite dal 1997 in avanti ci devono oggi stupire gli
studi clinici e le 3 indicazioni del Bevacizumab?
NO
Criticità:
Cosa significa post progressione? Nessuno ci spiega nel TML il tipo, il
volume e l’organo di progressione
Bobrie et al. Cancer Res, 2012
Koontongkaew et al., Journal of Cancer, 2013
Bevacizumab
BEVACIZUMAB
ALL
LIFE
LONG
Bevacizumab
Sulle basi molecolari fornite dal 1997 in avanti ci devono oggi stupire gli
studi clinici e le 3 indicazioni del Bevacizumab?
NO
Criticità:
Cosa significa post progressione? Nessuno ci spiega nel TML il tipo, il
volume e l’organo di progressione
Sospensione del Bevacizumab quando siamo nel caso di:
1)“microenvironment resistance” Æ ruolo degli esosomi (Rab27a)
???, resistant carcinoma associated fibroblasts (CAFs) ???
2)“microenvironment independent tumor growth” Æ misura
del flusso e densità vascolare intratumorale ???
Bobrie et al. Cancer Res, 2012
Koontongkaew et al., Journal of Cancer, 2013
Bevacizumab
Let’s come back to the Lab
Boehm et al. Nature, 1997
Bevacizumab Predictive factors
Investigated determinants:
•KRAS, BRAF and p53 mutational status;
• P53 and thrombospondin-1 tissue expression;
• VEGF epithelial and stromal expression;
• Microvascular density
• VEGF and VEGFR SNPs
• VEGF plasma levels
Ellis, ASCO 2010
VEGF -1498 C/T SNP: a retrospective experience
BEVACIZUMAB GROUP
CONTROL GROUP
-1498 T/T (N=29) median PFS: 7.5 months
-1498 T/T (N=25) median PFS: 8.6 months
-1498 C/T (N=60) median PFS: 10.5 months
-1498 C/T (N=55) median PFS: 8.2 months
-1498 C/C (N=22) median PFS: 12.8 months
-1498 C/C (N=27) median PFS: 8.0 months
Logrank test p= 0.0046
Logrank test p= 0.662
Loupakis et al. ESMO 2009
Prospective evaluation of candidate SNPs of
VEGF/VEGFR pathway
Prospective validation trial in mCRC pts treated with first-line
FOLFIRI+ BV to detect a HR for PFS of 1.7 for VEGF rs833061 T/T
compared to C- variants
Four-hundred-twenty-four pts included. At a median follow up of 24
months, median PFS was 10.5 months.
At the univariate analysis, no differences in PFS according to VEGF
rs833061 C/T variants were observed (p=0.38).
Among analyzed SNPs, only VEGFR2 rs12505758 C- variants (n=118)
were associated to shorter PFS compared to TT (n=306) (HR: 1.40
[95%CI: 1.07-1.84], p=0.015).
In the multivariate model, this association retained significance (HR:
1.402 [95%CI:1.079-1.822], p=0.012), that was lost by applying multiple
testing correction.
Conclusions: This prospective experience failed to validate the
hypothesized predictive impact of VEGF rs833061 variants.
Loupakis et al. ASCO 2012
Bevacizumab
Let’s come back to the Lab
Boehm et al. Nature, 1997
Bevacizumab
Il microambiente è il DRIVER del Bevacizumab
Studi sul microambiente dovrebbero moltiplicarsi, ve ne sono pochi, è
molto difficile condurli e potenziarli statisticamente per l’alto numero di
variabili
Bevacizumab inutile in adiuvante, perché?
E’ assente il driver di efficacia
Il concetto di “Time Related Efficacy” presente nello studio americano
adiuvante (NSABP C-08) non è altro che l’implementazione dei dati
molecolari discussi e rinforza il concetto di mantenimento e utilizzo in
post-progressione in caso di malattia presente anche microscopica
Allegra et al. JCO, 2010
mAb anti EGFR: Caratteristiche, Meccanismo d’azione, vantaggi selettivi
Cetuximab
T1/2: 5-7 giorni, somministrazioni
settimanali, ogni 2 settimane possibili
Affinità recettoriale EGFR: 0.30 nM
– IgG1 mAb
– Proteina Chimerica: Domini costanti di una molecola IgG umana combinati con
regioni variabili murine attraverso una fusione trangenica dei geni immunoglobulinici
Panitumumab
– IgG2 mAb
Completamente umanizzato:
T1/2: 3,6 – 10,9 giorni,
somministrazioni settimanali, ogni
2 wks, 3 wks??
Affinità recettoriale EGFR: 50 pM
Innesto all’interno di una struttura umana, di regioni CDR umane, selezionate per il riconoscimento
specifico dell’antigene scelto
Yang XD, et al. Crit Rev Oncol Hematol. 2001
mAb anti EGFR: Caratteristiche, Meccanismo d’azione, vantaggi selettivi
Principale Classico Meccanismo d’azione Cetuximab/Panitumumab e EGFR
Legame sul dominio III di una
“tethered sEGFR molecule”
Migliore inibizione classica sul dominio: Panitumumab
Panitumumab
Panitumumab biologicamente
perfetto sul dominio
Diverso significato
biologico/molecolare
Li et al., Cancer Cell, 2005
L’imperfezione come qualità
Cetuximab
CETUXIMAB
1) Minore affinità di legame con EGFR (rispetto
al Panitumumab) con EGFR
2) Interazione e sensibilità al microambiente
3) Maggiore possibilità di reazioni anafilattiche o
anafilattoidi (ordine del 2-3%)
4) Minore emivita
1) Maggiore variabilità di bersaglio
2) Legami stabili e scindibili solo con degradazione
3) Utilizzato meccanismo antitumorale ADCC
Ottima Qualità
Bio/Oncologica
4) Maggiore versatilità molecolare (Dose Intensity, Tossicità)
L’iperselettività come qualità
PANITUMUMAB
1) Altissima affinità di legame con EGFR
Panitumumab
2) Rapida internalizzazione e assente downregulation
proteolitica del complesso EGFR/Mab
3) Minore possibilità di reazioni anafilattiche o
anafilattoidi (max 1%)
4) Maggiore emivita
1) Interazione con recettori con mutazioni specifiche e
diverse da quelle inibite dal Cetuximab
Ottima e differente
3) Ritardo di acquisizione delle resistenze
Qualità Bio/Oncologica
4) Rapidità d’azione (Duillard, ESMO 2012)
Quali altri meccanismi d’azione?
CETUXIMAB
Internalizzazione del complesso recettore EGFR /Cetuximab e
downregolation della EGFR espressione
• Riespressione EGFR
EGFs e TGF-α
• Trasporto EGFR al
nucleo e attivazione
DNA-PK (DNA riparo)
Endosoma PH da
≈7Æ≈5
Scissione
Cetuximab
Endosoma PH da
≈7Æ≈5
Ferguson et al., 2003
Shiqing et al., Cancer Cell, 2005
Dittmann et al., J Biol Chem, 2005
• Effetto proliferativo
degli EGFs e sEGFR
Lisosoma
• Downregulation
EGFR (fisica e
proteolitica)
• Nessun effetto
proliferativo
sEGFR
Quali altri meccanismi d’azione?
PANITUMUMAB
Internalizzazione del complesso recettore EGFR /Panitumumab e
downregolation della EGFR espressione
• Rapida
internalizzazione
• Assenza di
degradazione
lisosomiale
Downregulation di EGFR (fisica e non proteolitica)
Possibilità di riespressione sulla membrana di EGFR
Assenza di inibizione DNA-Protein Kinasi di riparo attivata dal trasporto
intranucleare di EGFR (meccanismo d’azione cruciale per la RT)
Yang XD, et al. Crit Rev Oncol Hematol. 2001
Messersmith et al., Clin Cancer Res, 2007
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Internalizzazione del complesso recettore/mAb e impatto sul clivaggio
proteolitico di EGFR
Downregulation proteolitica di EGFR /
minore espressione EGFR su membrana
Assente downregulation proteolitica di EGFR /
inalterata espressione EGFR su membrana
-
+/-
By EGFR ubiquitination and degradation
and using Src kinase
CETUXIMAB/ EGFR
PANITUMUMAB/ EGFR
Sebbene l’ EGFR downregulation è un meccanismo di incremento di
efficacia, il perdurare di tale pathway potrebbe comportare resistenza
Imai et al., Nature Review, 2006
Lu et al., Cancer Res, 2007
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Citotossicità complemento/dipendente (CDC/CDCC) e citotossicità
cellulare Ab dipendente (ADCC)
CDC (complementdependent cytotoxicity ):
Dopo il legame del mAb, il
fattore del complemento
interagisce con la regione
costante CH2 del mAb la
quale porta all’attivazione
della cascata proteolitica
classica del complemento
formando i “membraneattack complexes (MAC) per
la lisi delle cellule tumorali
Imai et al., Nature Review, 2006
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Citotossicità complemento/dipendente (CDC/CDCC) e citotossicità
cellulare Ab dipendente (ADCC)
CDCC (complementdependent cell- mediated
cytotoxicity ): C3b generato
durante la CDC reazione
funziona come una opsonina
per facilitare fagocitosi e
citolisi attraverso
l’interazione con il C3b
recettore su macrofagi e NK
Imai et al., Nature Review, 2006
Quali altri meccanismi d’azione?
CETUXIMAB
Citotossicità complemento/dipendente (CDC/CDCC) e citotossicità
cellulare Ab dipendente (ADCC)
ADCC (antibody-dependent
cellular cytotoxicity):
Macrofagi e cellule NK
vengono reclutate e
interagiscono con la regione
CH3 del mAb attraverso il
loro FcγRIIIa espresso. Le
cellule tumorali ricoperte da
mAb e cellule immunitarie
sono fagocitate dai macrofagi
o vengono citolisate dalle NK
Regolazione neg effettuata da
FcγRIIb sempre espresso dai
macrofagi
Imai et al., Nature Review, 2006
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Citotossicità complemento/dipendente (CDC/CDCC) e citotossicità
cellulare Ab dipendente (ADCC)
IgG1 e IgG3 possono attivare la pathway classica del complemento e
interagire con Fcγ recettori; Non particolarmente le IgG2. In particolare
IgG4 non possono attivare la via del complemento
CDC/CDCC e ADCC:
CDC/CDCC e ADCC:
Cetuximab
Panitumumab
OK/OK
NI/NO
Ci sono dati preclinici forti che suggeriscono CDC/CDCC e ADCC come
importanti meccanismi d’azione antitumorali
Rivera et al., Acta Oncologica, 2008
Lo et al., AACR-NCI-EORTC Int Conf
Mol Targets Cancer Ther, 2003
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Inibizione dei recettori mutati o disregolati
(differenti mutazioni e disregolazioni inibite)
“Untethered Monomers”: Cetuximab previene la
formazione di tali forme (vII) riducendo il legame
dei ligandi ad alta affinità sia sul dominio I che
III anche con un cambio di conformazione sterica
Cetuximab inibisce la forma vIII dell’EGFR attraverso il
legame FabVH/Dominio I EGFR e prevenendo il dominio II
dalla conformazione sterica necessaria per la dimerizzazione
Li et al., Cancer Cell, 2005
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Blocco eterodimerizzazione tra EGFR/IGF-1R e blocco della via di
trasduzione del segnale di IGF-1R
L’attivazione di IGF-1R attraverso l’eterodimerizzazione EGFR/IGF-1R
e la conseguente espressione di Survivina media la resistenza al Gefitinib
nelle NSCLC cells
H460: Cellule resistenti al gefitinib
Cetuximab/Panitumumab impediscono tale eterodimerizzazione bloccando
anche tutta la via a valle di IGF-1R con affinità e modalità differente
Morgillo et al., Clin Cancer Res, 2007
Karamouzis et al., Trends Mol Med, 2006
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Blocco eterodimerizzazione tra EGFR/PDGFR e blocco della via di
trasduzione del segnale di PDGFR-β
Cetuximab inibisce
eterodimerizzazione naturale
EGFR/PDGFR-β a dosi
crescenti proporzionalmente
all’espressione di PDGFR-β
Cellule UM-UC5 overesprimenti PDGFR-β sono resistenti al Cetuximab
probabilmente per spiazzamento mAb dal recettore; Panitumumab
meccanismo elettivo vista la sua più alta affinità recettoriale
Brown et al., AACR meeting, 2006
Ingram et al., Curr Mol Med, 2006
Karamouzis et al., JAMA, 2007
Black et al., Urologic Oncology, 2007
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Blocco eterodimerizzazioni tra EGFR/IGF-1R e EGFR/PDGFR-β
rappresentano una VIA COMUNE
Blocco eterodimerizzazione tra EGFR/Recettori per Molecole Ormonali e
blocco trasduzione del segnale ormonale “indiretto”
PELP1/MNAR
Modulatori attività ormonale estrogenica
Karamouzis et al., JAMA, 2007
Gururaj et al., Clin Cancer Res, 2006
Quali altri meccanismi d’azione?
CETUXIMAB/PANITUMUMAB
Blocco eterodimerizzazione tra EGFR/Recettori per Molecole Ormonali e
blocco trasduzione del segnale ormonale “indiretto”
Ormonoresistenza
Cetuximab
Panitumumab
Blocco eterodimerizzazione potrebbe significare restituita ormonoresponsività (Ca mammella / Ca prostata)
Jakobovits et al., Handb Exp Pharmacol, 2008
Gadducci et al., Crit Rev Oncol Hematol, 2006
Ross et al., Cancer Metastasis Rev, 2005
Quali altri meccanismi d’azione?
CETUXIMAB
Modificazione della matrice extracellulare
Meccanismo ADCC
Cetuximab induce infiltrazione macrofagica
del tumore
1
TAM: Macrofagi Tumore Associati
(1) Degradazione delle metallo-proteinasi di matrice richieste per
l’adesione e metastatizzazione delle cellule tumorali
Panitumumab: nessuna modificazione ECM
Assente ADCC
Kim et al., Clin Cancer Res, 2006
Frieze et al., Ann Pharm, 2006
Shih et al., J. Cancer Mol, 2006
Riassumendo
CETUXIMAB VS PANITUMUMAB
Meccanismi d’azione misconosciuti non da inibizione classica della
pathway di EGFR
Cetuximab
Panitumumab
Internalizzazione del recettore
SI
SI (+ radido)
• Dowregulation EGFR fisica
SI
SI (+ rapido)
• Dowregulation EGFR proteolitica
SI
NO (vantaggio
resistenze acquisite)
• Inibizione DNA PK (riparo DNA)
SI (vantaggio
RT)
NO
CDC/CDCC
SI
NI (IgG2 non particolarmente attive
nell’attivare complemento)
ADCC
SI
Inibizione recettori mutati o disregolati
Non è Multitargets
No azione su MI
> Affinità
Rec
SI Multitargets SI (diversa
affinità)
Reale
¾Peculiarità di
Azione anche MI
funzione
Blocco EGFR dimerizzazione con IGF1R, PDGFR, Rec. Ormonali
Interazione con matrice extracellulare
NO
SI
SI
SI
NO
Cosa spiegano tali meccanismi d’azione?
Cetuximab e Panitumumab sono 2 risorse da sfruttare con intelligenza e
ancora tanto da studiare. ---- Non sono farmaci in concorrenza ---Potrebbe essere cruciale una selezione di pazienti anche sulla competenza
del complemento o su forme particolari del recettore di EGFR vII, vI, vIII
per la scelta farmacologica e/o decisione di linea terapeutica
Cetuximab viste le caratteristiche biologiche neoplastico/specifiche e
microambientali è allo stesso modo del Bevacizumab un ottimo candidato
ad essere studiato in mantenimento e post-progressione
Cetuximab a fallimento di Panitumumab: un’opzione non da scartare,
potenzialmente efficace su più target
Panitumumab a fallimento di Cetuximab: un’opzione non da scartare
Imai et al., Nature Review, 2006
Helbling et al., Ann Oncol, 2007
Mutation in the EGFR extracellular domain
Cetuximab-resistant cells from the highly sensitive human
mCRC cell line DiFi (which is wild-type for KRAS, BRAF and
PI3K and has an amplification of EGFR)
These cells continuously treated with cetuximab. Five months
after beginning treatment, was isolated DiFi-derived cetuximabresistant clones (DCR) (DCR 7, DCR 9 and DCR 10)
Montagut et al, Nature Medicine, Jan 2012
Mutation in the EGFR extracellular domain
No detect mutations in KRAS, BRAF or PIK3CA or loss of
PTEN expression in the DCR clones
Viability and EGFR signaling in the DCR clones were
effectively decreased by treatment with the antibody
panitumumab
Montagut et al, Nature Medicine, Jan 2012
Mutation in the EGFR extracellular domain
Acquired EGFR ectodomain mutation (S492R) that
prevents cetuximab binding and confers resistance to
cetuximab
In Cells carrying the S492R mutation, only panitumumab
blocked the activation of EGFR
Comparison of the abilities of cetuximab and panitumumab to
interact with WT EGFR and the S492R EGFR mutant in vitro
Montagut et al, Nature Medicine, Jan 2012
Mutation in the EGFR extracellular domain
Clinical Phase
Examination pre- and post-therapy specimens from ten
individuals with mCRC who experienced disease progression
after a prior response to cetuximab with chemotherapy
Detection the S492R mutation in two subjects. The detection of
the acquired EGFR S492R mutation led investigators to offer
him panitumumab according to the approved monotherapy
schedule
Montagut et al, Nature Medicine, Jan 2012
Cetuximab come terapia di mantenimento della risposta nel mCRC
Concettualmente, perchè no?
Biologicamente, assolutamente si:
-
Malattia colorettale policlonale ed eterogenea
Farmaco interagisce con il microambiente come il Bevacizumab
Approvato e strutturato per altre patologie
Fattibilità, si:
-Con qualche stratagemma
Eppure il mantenimento non è formalmente strutturato
ERBITUX + chemioterapia a base di platino
(Studio EXTREME) Disegno dello studio
Mantenimento
Studio multicentrico, di
fase III, randomizzato
(n=442)
Chemioterapia a base di platino
+ ERBITUX
(n=222)
ERBITUX
fino alla progressione di
malattia o tossicità
inaccettabile
Chemioterapia a base di platino
(n=220)
Chemioterapia a base di platino
Cisplatino 100 mg/m2 O carboplatino AUC 5,
giorno 1
5-FU 1000 mg/m2/giorno, giorni 1–4
cicli di 3 settimane, fino a 6 cicli
Vermorken et al. New Engl J Med 2008;359:1116–1127
ERBITUX
Dose iniziale di 400 mg/m2
poi 250 mg/m2 ogni settimana
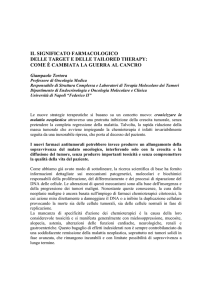
EXTREME: Overall survival
1.0
0.9
|
| ||
|
|
|
| |
Survival probability
0.8
Chemotherapy only
||
|
0.7
HR [95%CI]: 0.80 [0.64–0.99]
p=0.04
|
0.6
10.1 months
0.5
0.4
0.3
0.2
7.4
months
|
|
|
| |
| |||| | | |
|
| ||
| | || | |
||
||
|| | | ||
||
| |||
|
| ||
|||
| | | | ||
| ||| | | |
| | | | | | || ||| |
0.1
Vermorken JB et al. N Engl J Med 2008;359:1116–1127
24
Cetuximab come terapia di mantenimento della risposta nel mCRC
Almeno 4 “strong evidences” in altri tumori che il mantenimento è utile
Nessun dato strutturato sul mCRC su quanto potrebbe aggiungere tale
strategia
Considerando che del Cetuximab/Panitumumab:
-Non conosciamo i meccanismi di non risposta specie nei K-RAS WT
-Non sappiamo la eventuale sequenzialità
-Non sappiamo stratificare biologicamente i pazienti
-Non conosciamo ruolo in mantenimento e Post progressione
Let’s come
back to the Lab
Mecca et al., Eur J Dermatol, 2012
Mesia et al., Ann Oncol, 2013
Colucci et al., Oncology 2010
Jensen et al., Cancer 2011
Argiris et al., JCO 2010
Cetuximab come terapia post-progressione
Strategia terapeutica ottimale nei pazienti con
tumore del colon-retto metastatico
K ras wild type: cetuximab in associazione con
FOLFIRI seguito dal FOLFOX +/cetuximab. Studio Multicentrico del GOIM
(Prot.2906 – CAPRI )
Metastatic wt KRAS CRC
*FOLFIRI +
CETUXIMAB
PD
R
A
N
D
O
M
I
Z
A
T
I
O
N
FOLFOX +
CETUXIMAB
FOLFOX
Sangue
basale per la determinazione dei
polimorfismi di EGF ,EGFR e FCγ EGFR
*FOLFIRI+Cetuximab until PD
FOLFOX+Cetuximab until PD
Plasma
per lo studio di 100 proteine microambintali
coinvolte nelle risposta e nella resistenza al
cetuximab
Aflibercept: Come superiamo la resistenza alla terapia anti VEGF ?
Aflibercept: Come superiamo la resistenza alla terapia anti VEGF ?
Aflibercept is a recombinant
fusion protein which acts as
a decoy receptor that binds
to:
- Vascular Endothelial
Growth Factor-A
(VEGF-A), VEGF-B and
placental growth factor
(PIGF-1 and 2)
- Binding sequences from
VEGF receptors 1 and 2
Aflibercept: Come superiamo la resistenza alla terapia anti VEGF ?
-
-
-
-
Expression of VEGFR1-2
on tumors, vessels, and
macrophages is high
sVEGFR1 expression in
plasma is high.
Expression of NRP1 on
tumor cells is also high
such as PIGF1 and 2
Expression of various other
angiogenic molecules,
including IL-8, bFGF,
PDGF-BB, PDGF-C,
VEGF-C, and VEGF-D.
Lambrechts D et al. JCO 2013;31:1219-1230
GI Cancer Updates
“VELOUR” Study
Author: J Tabernero et al
Reviewed by: Dr. Scott Berry
Date posted: October 27, 2012
www.OncologyEducation.com
Study Design
N=1200
Primary
Outcome:OS
Aflibercept 4 mg/kg IV, day 1 +
FOLFIRI q2 weeks
R
mCRC
Previous
Oxaliplatin
Based Tx
FOLFIRI q2 weeks
www.OncologyEducation.com
RESULTS
FOLFIRI
FOLFIRI+
AFLIBERCEPT
p-value
Response
Rate (%)
11.1
19.8
P= 0.0001
PFS/TTP
(median,
mos)
4.67
6.90
P=0.00007
OS
(median,
mos)
12.06
13.5
HR=0.82
P=0.0032
Van Cutsem D et al. JCO 2012
www.OncologyEducation.com
Overall Survival: Patients with or
without Prior Treatment with
Bevacizumab - ITT Population
Placebo/ FOLFIRI Aflibercept/FOLFIR
Median (mos)
I
N = 614
Median (mos)
N = 612
12.1
13.5
No
12.4
13.9
Yes
11.7
12.5
All Patients
P-value for
interaction
Prior BEV
P=0.7231
Interaction between “treatment arm” and “prior
bevacizumab” factor was not significant at the 2-sided 10%
level (p = 0.7231).
Improvement in OS was consistent regardless of prior
treatment with bevacizumab
Van Cutsem D et al. JCO 201216
www.OncologyEducation.com
Aflibercept: Un Farmaco studiato bene!!! ---per ora---
Prova di principio: SI
Studi di fase preclinica e clinica con PK e PD: SI
Studi di interazione e di sinergismo molecolare con IRI e OX: Si
Studio di interazione con OX
non è così schiacciante!!!!
ASCO 2010
Studi di fase II e III prima e seconda linea: SI (vd AFFIRM Trial)
Wang et al. Med. Oncol. 2012
Aflibercept: Cosa manca?
Studi in mantenimento e post progression: in vitro e preclinici in vivo.
Perché non iniziare da subito?
Ricordiamoci che la storia del Beva mantenimento e post-progressione è
iniziato concettualmente nel 1997
Studi di combinazione con altri antiangiogenetici (i.e. Inibitori
Neuropilina 1 -NRP-1-)
Conclusioni