[PDF")
Clinica Pediatrica Università degli Studi Parma
Bernasconi S.
Boscherini B.
Cianfarani S.
Cohen A.
Lala R.
Maghnie M.
Panei P.
Pocecco M.
Ravaglia A.
Bernasconi S. Boscherini B. Cianfarani S. Cohen A.
Lala R. Maghnie M. Panei P. Pocecco M. Ravaglia A.
Finalità :
1 ) Rivedere la nota 39 sulla base dell’esperienza maturata
dopo la precedente versione;
2) Proporre le proposte al vaglio di associazioni,società
scientifiche, gruppi di esperti;
3) Fornire all’AIFA una proposta finale di revisione la più
ampiamente condivisa.
Punti fondamentali :
-alterata funzione del gene SHOX
Descrizione delle richieste valutate
anni 2008-2012
Centro richiedente
%
centri RER
centri extraRER
totale richieste trattamento
numero
52
3
55
Sesso dei soggetti in età evolutiva con richiesta di trattamento
Femmine
Maschi
totale richieste trattamento
numero
23
32
55
%
Diagnosi dei soggetti
SGA con malattia rara o sospetto o note sindromiche
SGA
totale richieste per soggetti SGA
alterazioni gene SHOX
deficit di attività biologica del GH
malattia rara
iposomia grave
totale richieste per bassa statura e normale secrezione GH
numero
8
19
27
2
3
8
15
28
%
15%
35%
49%
4%
5%
15%
27%
51%
95
5
100
42
58
100
Punti fondamentali :
-alterata funzione del gene SHOX
- fase di transizione
Punti fondamentali :
-alterata funzione del gene SHOX
-fase di transizione
- GHD
A new preparation has recently become
available, the Second International Standard for somatropin
(a recombinant DNA–derived human GH, international
standard (IS) 98/574), and is being used by
manufacturers for standardization of GH assays. It is
available from National Institute of Biological Standards
and Control (NIBSC). This material is of high
purity (96% 22-kDa GH) with desirable characteristics
(bioactivity, stability, availability, and so forth)
The ideal assay should use antibodies of high affinity
and specificity. Assays should be specific for the 22kDa form of human GH. Reproducibility may be the
most critical near the lower limit of the analytical interval
Growth curve of a boy with constitutional delay
showing slower growth in the peripubertal time and
then achievement of the normal range by the end of
the growth process. The growth velocity curve is
shown with a more attenuated and lower increase at
puberty (Ghizzoni, Street 2007)
Età ossea ritardata
L’inizio della pubertà correla
maggiormente con l’età ossea che
con l’età cronologica.
PROPOSTA
Al di sotto di 2 anni di vita non è necessario
praticare i test farmacologici se la RMN ha
dimostrato una anomalia della adenoipofisi
associata a quella del peduncolo o/e della
neuroipofisi in un bambino con progressiva
decelerazione della velocità di crescita
Punti fondamentali :
-alterata funzione del gene SHOX
-fase di transizione
- GHD
-Deficit staturali non GHD
Esclusa attraverso polisonnografia
This demonstrates that
although polysomnography
is advised before starting GH
treatment, particularly in the
presence of snoring or
obesity, a normal result
cannot guarantee 100%
safety.
Nevertheless, because 75% of
deaths of GH-treated children
occurred in the first 9 months after
commencing treatment, we could
not eliminate a possible
aggravating role of GH at the
start of treatment emphasizing the
need for careful management of
these patients.
Andamento terapie autorizzate
Situazione a novembre 2012
Andamento casi autorizzati
numero
%
prosecuzioni terapia
28
65%
trattamenti interrotti o non intrapresi
15
35%
totale richieste autorizzate
43
100%
Trattamento con GH nei casi autorizzati dalla Commissione
prevalenza trattamento 2012 (n° trattati*1000 residenti 0-18 anni)
0,040
incidenza trattamento 2012 (n° pazienti incidenti*1000 residenti 0-18 anni)
0,016
Grazie per l’attenzione
Dipartimento Universitario Ospedaliero
Responsabile UOC di Endocrinologia e Diabetologia
31
La storia del GH DAL 1985…………
AGHD
GHD
CRI
1985
Microsoft
Windows
1990
TS
AIDS
1995
Prozac
DVDs
SGA
PWS IS
S
Transizion
e
SHO
X
2000
Campioni
Del mondo
2004
Ben XVI
Monti
Berlusconi
Cossiga
Prodi
32
La storia del GH DAL 1985…………
AGHD
GHD
CRI
1985
Microsoft
Windows
1990
TS
AIDS
1995
Prozac
DVDs
SGA
Transizion
e
SHO
X
21-2-2011 . AIFA
(autorizzazione)
PWS IS
S
2000
Campioni
Del mondo
2004
Ben XVI
Monti
Berlusconi
Cossiga
Prodi
33
Scopi del Trattamento
Normalizzazione del ritmo di
crescita
Raggiungimento di una
statura adulta normale
Correzione delle eventuali
anomalie metaboliche
34
Il gene SHOX
35
La regione pseudoautosomale
PR48
Cr.Y
OA1
PPEF1
11.2
SRY
11.1
UTY
11.2
SMCY
PAR1
SHOX
12
1.037
SYBL1
983
803
AR
11.3
238
Cr.X
CFS2RA
PDCD8
IL3RA
L1CAM
SYBL1
ASMT
36
•
E’ ben nota la relazione tra statura e cromosomi
sessuali, dimostrata dalle caratteristiche fenotipiche di
alcune sindromi cromosomiche
• Il numero dei cromosomi X influenza la statura: un
aumento determina alta statura (es. sindrome di
Klinefelter), viceversa il deficit determina bassa statura
(es. sindrome di Turner)
• Diversi studi di citogenetica su delezioni terminali del
braccio corto dei cromosomi X e Y e correlazioni
genotipo-fenotipo hanno suggerito che uno o più geni
rilevanti per la crescita risiedano nella regione
pseudoautosomale (PAR 1) dei cromosomi sessuali
37
SHOX is a height controlling gene
Klinefelter
38
Gene SHOX
• Rao dimostrò che un intervallo di 170 kb era
deleto in 36 individui con bassa statura portatori
di riarrangiamenti cromosomici su Xp22.3 e
Yp11.3.
• Il gruppo di Ellison isolò un gene dalla stessa
regione.
• Entrambi i gruppi suggerirono che esso potesse
essere coinvolto nel fenotipo della bassa statura
della sindrome di Turner.
• Il gene fu chiamato Short Stature Homeoboxcontaining gene (gene della bassa statura
contenente homeobox – SHOX)
39
Il gene SHOX
• L’aploinsufficienza di SHOX o la completa
perdita di funzione, provoca una atipica
proliferazione
e
differenziazione
dei
condrociti alterando l’equilibrio dei due
processi nei centri di ossificazione.
• Tale sbilanciamento è responsabile del
ritardo di crescita longitudinale dell’osso
lungo con modalità differenti tra periodo
embrionale e periodi successivi.
40
Disturbi associati a deficit del gene
SHOX
• Sindrome di Léri-Weill (discondrosteosi di
Léri-Weill)
• Displasia mesomelica di Langer
• Sindrome di Turner
• Bassa statura idiopatica
41
Accorciamento mesomelico delle ossa lunghe
schke R.J.& Rappold G. Current Opinion in Genetics & Development
42
• Grave bassa statura
• Displasia scheletrica severa caratterizzata da riduzione dei segmenti
mediani degli arti (mesomelia)
• Anomalie scheletriche associate: ipoplasia mandibola, radio, ulna,
deviazione ulnare mani
SHOX expression in human embryos begins
26 days post-conception
Human Embryo at Cs 19
43
44
SHOX governs intermediate limb differentiation in
developing limb of human embryo
> Cs13
SHOX2
SHOX
SOX9
> Cs14
(HOX 10)
(HOX 11)
Embryonic stage
Cs18
41 days p.c.
Marc Clement-Jones
45
Statura nei bambini con anomalie del gene
SHOX
Ross JL et al J Pediatr 2005
46
Madelung Wrist Deformity
• Avambraccio corto
• Incurvamento latero-dorsale del radio
• Ipoplasia distale dell’ulna dislocata in modo
dorsale
• Ampliamento variabile dello spazio
interosseo tra radio e ulna
• Limitata mobilità di gomito e polso
47
SHOX-D
Avambraccio corto
Cubito valgo
Deformità di Madelung
48
LERI-WEILL DISCONDROSTEOSI
Ipertrofia muscolare
Curvatura tibia
A a SX bambino sano, a DEX fratello con LWS
Ross JL et al J Pedaitr 2005
49
Frequenza dell’aploinsufficienza di
SHOX e fenotipo
BSI
2-5%
BSI
disarmonica
22%
Madelung
67%
LERI-WEILL
74.5%
TURNER
45XO
100%
50
Bassa statura idiopatica
Frequenza delle mutazioni di SHOX nella BSI
e tecniche di indagine genetica
Autore/anno
Frequenza mutazioni %
Metodologia
Rao, 1997
1.1%
SSCP + MS
Binder, 2000
1.5%
SSCP + MS (>2)
Rappold, 2002
2.4%
SSCP + FISH
Stuppia, 2003
12.5%
FISH +
Sequenziamento
Huber, 2006
15%
MS + Sequenziamento
(Completo PAR1)
Jorge, 2007
3.2%
MS + FISH +Sequenziamento
Rappold, 2007
2.2%
MS + FISH +
SNP screening in 275
51
52
ISS
(n=740)
Point mutations
SHOX gene
PAR1 deletions
including SHOX
PAR 1 deletions
downstream SHOX
Total
5
(0.7%)
23
(3.1%)
8
(1.1%)
36
(4.9%)
J Med Genet 2009
Frequenza delle mutazioni di SHOX nella
BSI ed Etnia
Autore/anno
Frequenza
mutazioni %
Provenienza geografica/Etnia
Rao, 1997
1.1%
Giappone / Asiatica (90%)
Germania / Caucasica
Binder, 2000
1.5%
Germania/Caucasica
Rappold, 2002
2.4 %
Giappone/Asiatica (70%)
Germania/Caucasica
Stuppia, 2003
12.5%
Italia/Caucasica
Huber, 2006
15%
Francia/Caucasica
Jorge, 2007
3.2%
Brasile/Caucasica (70%)+
Indiano-americana +Africana
Rappold, 2007
2.2%
Europa / Caucasica (84%)
Giappone / Asiatica
53
CRITERI DI SELEZIONE
DEI PAZIENTI CON BSI
L’uso del
rapporto
“altezza
seduta/altezza”
63 bambini
: statura < -2 DS
cariotipo normale,
non evidenza di anomalie (SH/H)
scheletriche, non
nel caso indice
né in parenti di 1°la
grado,
come criterio
diMadelung
selezione
aumenta
frequenza
Rx mano e polso normale, escluse patologie organiche e GHD
dello SHOX deficit fino al 22% e dovrebbe essere
usato per selezionare i bambini ISS in cui ricercare
le anomalie Misurazione
del gene
SHOX
di statura
eretta, statura seduta, arm span
Calcolo del rapporto Statura seduta/Statura eretta (SH/H) in SDS
FISH +Sequenziamento SHOX
2 Pazienti positive per mutazione puntiformi di SHOX 0 = 3.2%
56 pazienti SH/H < 2 SD
Nessuno SHOX-D
9 pazienti SH/H > 2 DS
2 SHOX-D = 22
%
54
55
56
57
58
59
Rapporto estremità-tronco
Somma
(span delle braccia + segmento inferiore)
=
Altezza seduta
Approssimazione matematica:
rapporto significativo
se inferiore a 1.95 + ½ altezza in metri
Binder G et al JCEM 2003; 88:4891-86
CRITERI DI SELEZIONE
DEI PAZIENTI CON BSI
Popolazione studiata: 1534 BSI (60% maschi)
Mutazioni SHOX: 34 pazienti (2.2%) (54% f e 46% m)
Delezioni complete o parziali: 77%
Familiarità per LWS o S. Langer nei pazienti SHOX-D (TH)
Correlazione genotipo-fenotipo:nei pz SHOX-D ↑ statura
seduta/statura eretta, ↑ avambraccio corto, ↑ circonferenze arti,
↑ BMI
60
Segni clinici in pazienti con BSI e
SHOX-D
Rappold et al,J Med Genet 2007
61
Caratteristiche antropometriche
di pazienti con BSI e SHOX-D
Rappold et al,J Med Genet 2007
62
63
QUANDO EFFETTUARE ANALISI
DELLO SHOX
Analisi di SHOX
quando score >7
Rappold et al, J Med Genet
2007
QUANDO EFFETTUARE ANALISI
DELLO SHOX
Analisi di SHOX
quando score >7
Rappold et al, J Med Genet
2007
64
Frequenza delle mutazioni di
SHOX nella Bassa Statura
Idiopatica
Variabile tra 1.1% -15 %
Variabilità legata a criteri di selezione della
popolazione studiata, numerosità del campione, etnia
Delezioni > mutazioni puntiformi; rapporto
variabile con le tecniche di indagine genetica
Forme sporadiche/familiari: 1/2 (Huber,2006)
Maggiore prevalenza nel sesso femminile (71%
Stuppia et al, 2003; 55% Huber et al, 2006; 54%
Rappold et al, 2007)
65
66
67
68
Deformità di Madelung
69
70
71
72
73
GH at a dose of 1.0 IU/kg/week
74
75
76
77
Blum et al, J Clin Endocrinol Metab 2007; 92:219-28
78
Blum et al, J Clin Endocrinol Metab 2007; 92:219-28
No terapia
GH terapia
Artralgia
Ginecomastia
2/25
0/12
3/27
1/12
Nevi cutanei
0/25
2/27
Otiti medie
1/25
1/27
Scoliosi
0/25
1/27
Non sono riportati gravi eventi avversi in soggetti con SHOX-D.
79
Height gains in response to Growth hormone treatment to final height are similar
in patients with SHOX deficiency and Turner syndrome.
Blum et al, Horm. Res. 2009; 71:167-73
80
Fattori che migliorano la statura adulta
• Inizio precoce della terapia con GH
• Alta statura ad inizio terapia
• Uso di dosi utilizzate per la ST
• Lunga durata della terapia con GH
• Somministrazione giornaliera
81
Deficit di SHOX: Take home message
La terapia con GH migliora la
statura in pazienti con SHOX-D
Risultati preliminari indicano che
la terapia combinata con GH e
GnRHa migliora la statura da
adulto
Non sono stati registrati effetti
collaterali di rilievo
82
IRCCS Giannina Gaslini
Department of Pediatrics
University of Genova
Nota AIFA 39
Aspetti Specifici: Età di Transizione
IV Convegno “ Il Trattamento con l’Ormone Somatotropo in Italia”
27 Novembre 2012 Roma
Mohamad Maghnie
[email protected]
[email protected]
Gazzetta Ufficiale N 270 del 18 Novembre 2010
Agenzia Italiana del Farmaco
Determinazione 29 Luglio 2010
Modifica alla Nota AIFA 39 di cui alla determinazione del 26 Novembre 2009
Età di Transizione
-Viene definita età di transizione quella compresa tra il momento del raggiungimento
della statura definitiva del soggetto trattato e l’età di 25 anni
•Al raggiungimento della statura definitiva non è più indicata la
terapia con GH nelle seguenti patologie:
–
–
–
–
sindrome di Turner;
insufficienza renale cronica
sindrome di Prader Willi;
Soggetti nati piccoli per età gestazionale (SGA);
Gazzetta Ufficiale N 270 del 18 Novembre 2010
Agenzia Italiana del Farmaco
Determinazione 29 Luglio 2010
Modifica alla Nota AIFA 39 di cui alla determinazione del 26 Novembre 2009
Età di Transizione
Al raggiungimento della statura definitiva la terapia con GH può essere
proseguita senza ulteriori rivalutazioni nelle seguenti patologie:
- deficit di GH causato da mutazione genetica documentata
- panipopituitarismo con difetto di secrezione ormonale multiplo di
almeno tre ormoni ipofisari.
-Al raggiungimento della statura definitiva la terapia con rGH negli altri
soggetti con deficit di GH può essere proseguita solo se presentano dopo
almeno un mese dalla sospensione del trattamento sostitutivo con rGH:
a) risposta di GH <6 μg/L dopo ipoglicemia insulinica (ITT);
oppure
b) risposta di GH <19 μg/L dopo test farmacologico con
GHRH+Arginina
GH testing not required for those with:
• A transcription factor mutation (e.g., POU1F1,PROP1, HESX1,
LHX3,
LHX4 )
• More than three pituitary hormone deficits
• Isolated GHD associated with an identified mutation (e.g., GH-1,
GHRH)
• For Non - GHD pediatric indications (e.g., Turners, SGA..) there is no
proved benefit of GH treatment in the adult; there is no indication
to evaluate GH status at the completion of growth
• All other patients should undergo GH testing after at least one month
off GH treatment
Suggested cut-off in transition period, based on present evidence is GH
peak < 6 g/L to ITT. Further validation required
Remarks:
• Arginine and clonidine not useful in the transition age
• Limitation for most tests is relative lack of validated
• Normative data based on age, gender and BMI
Cut off of 5 µg/L after ITT confirmed also by the 2009 AACE consensus
and by the 2011 endocrine society guidelines
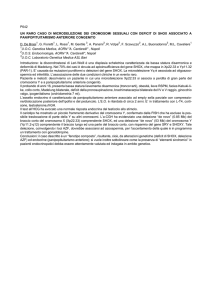
Figure showing the process of re-evaluation of GH and IGF-I levels
at the end of growth in those with GH deficiency diagnosed in
childhood
Diagnosed GHD in childhood – Now at the end of growth and puberty
Discontinue GH for at least 1 month+
High likelihood severe GHD
Low likelihood severe GHD
Measure serum IGF-I
Undertake GH stimulation
test, measure serum IGF-I
≤ -2SD –
diagnosis
confirmed
≥ -2SD –
undertake GH
stimulation test
Low peak GH*
Normal
peak GH*
Restart GH
Both low –
diagnosis
confirmed
Both
normal
Tests
discordant
Restart GH
Discharge unless
risk of evolving
endocrinopathy
Follow-up
Reconsider
diagnosis
* Peak GH < 5 µg/L
+For those with severe congenital hypopituitarism, GH
can be continued without interruption
Clayton P et al. Eur J Endocrinol 2005; 152:165-170
Defining a Disease……
ISSUES
• The ITT adopted cutoff by the 2007 Consensus was established in a small
cohort of 26 patients (39 controls). The GH of 6.1 µg/L was the highest
observed value in the patients and the lowest in the controls.
Defining a Disease……
ISSUES
• The ITT adopted cutoff by the 2007 Consensus was
established in a small cohort of 26 patients (39 controls). The
GH of 6.1 µg/L was the highest observed value in the
patients and the lowest in the controls.
• ITT contraindicated in patients with ischemic heart disease
or with seizures
• GHRH + Arginine stimulates both hypothalamus and
pituitary and may miss GH deficiency due to hypothalamic
disease (CRT), and is markedly influenced by BMI.
• GH <19 μg/L was obtained in subjects with BMI<25
kg/m2
• Discordants ? Metabolic consequences? Rescue/Puberty?
Tasks after Adult Height Achievement
Clinical Decisions
• Who do we Retest?
• When do we Retest?
• How do we Retest?
• Who do we consider Treating?
• Follow-up and End points?
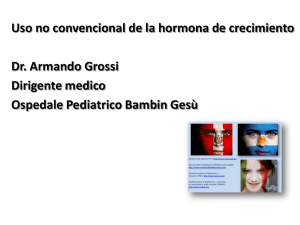
ROC curve analyses of peak GH to ITT (A), 12-h SNGH (B) and IGF-I SDS (C), in the entire study population (♦) and in
74 subjects after exclusion of those with hypogonadotropic hypogonadism treated with oral estrogens (▴).
ROC analysis showed the best
Diagnostic Accuracy for peak of
5.62µg/L
Secco A et al. JCEM 2009;94:4195-4204
©2009 by Endocrine Society
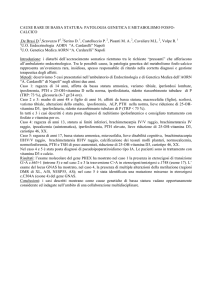
Distribution of 79 subjects according to their hormonal status (▵, IGHD; ▴, MPHD with one additional defect; •, MPHD with two or
more additional defects), MRI findings, likelihood of permanent GHD, and diagnostic cutoffs indicated by ROC analysis for peak
G...
7 patients with HLGHD showed
a peak > 5.62 µg/L
Secco A et al. JCEM 2009;94:4195-4204
©2009 by Endocrine Society
GHRH Plus Argine Test
Publication
BMI<25 kg/m2
BMI 25-30 kg/m2
BMI ≥30 kg/m2
Corneli et al. 2007/
19.0
ND
ND
GHRS 2007/Adults
<11.0
<8.0
<4.0
AACE 2009/Adults
<11.0
<8.0
<4.0
Endo Soc
2011/Adults
<4.1
<4.1
<4.1
Effects of BMI on Stimuated GH Secretion
Clonidine
173 children
Loche et al, Clin Endocrinol, 2011
Effect of BMI on GH responses to different stimuli
Clonidine, Arginine and ITT
838 children
Multivariate regression analysis
Indipendent variables:
H-SDS, Pubertal Status, BMISDS, IGF1-SDS and Type of
B
P
BMI-SDS
-1.41
<10-5
Height-SDS
-1.21
<10-4
IGF-I SDS
0.99
<10-4
Type of stimulus
0.89
0.01
adjusted
R2
0.11
Unpublished
Di Iorgi et al, ENDO 2012
A plot showing the significant negative correlation between the peak GH responses to the
combined GHRH + AST in patients and the length of follow-up since irradiation.
Darzy K H et al. JCEM 2003;88:95-102
©2003 by Endocrine Society
Tasks after Adult Height Achievement
Clinical Decisions
• Who do we Retest?
• When do we Retest?
• How do we Retest?
• Who do we consider Treating?
• Follow-up and End points?
• Benefits of GH replacement throughout life have been
demonstrated. Thus, GH status should be reevaluated in
the transition age for continued GH replacement to
achieve full somatic development.
GH therapy should be continued after
completion of adult height to obtain full
skeletal/muscle maturation during the
transition period
JCEM, June 2011
Effect of Discontinuing GH Treatment at Final Height
•
•
•
•
•
•
•
Reduced muscle mass
Reduced bone mineral content
Reduced body mass
Reduced IGF-I
Increase in fat mass
Deterioration of the lipid profile
Deterioration of fibrinogen levels
Effect of GH Replacement In Transition
•
•
•
•
•
Increase in muscle mass
Decrease in fat mass
Increase in bone mineral content
Increase in bone mineral density
Improved QOL
FIG. 1. Flow chart showing the cohort of patients with childhood-onset GHD subdivided
according to the peakGH response cutoff point and MRI features at the time of adult height
achievement
di Iorgi, N. et al. J Clin Endocrinol Metab 2007;92:3875-3884
Copyright ©2007 The Endocrine Society
Structural & Pituitary Abnormalities in Congenital GH Deficiency
Posterior Pituitary Site
EM
PI
IP
IA
Waist circumference, serum total cholesterol, and serum fibrinogen represented as mean ± sd in the 13 patients at baseline and
after 2-yr follow-up, compared with the control group of 20 unaffected subjects.
di Iorgi N et al. JCEM 2007;92:3875-3884
©2007 by Endocrine Society
Correlations between IGF-I SDS values and peak GH responses to ITT with serum cholesterol at 2-yr followup in the 13 studied patients.
di Iorgi N et al. JCEM 2007;92:3875-3884
©2007 by Endocrine Society
Secco A et al. JCEM 2009;94:4195-4204
Tasks after Adult Height Achievement
Clinical Decisions
• Who do we Retest?
• When do we Retest?
• How do we Retest?
• Who do we consider Treating?
• Follow-up and End points?
FIG. 1. Flow chart showing the cohort of patients with childhood-onset GHD subdivided
according to the peakGH response cutoff point and MRI features at the time of adult height
achievement
di Iorgi, N. et al. J Clin Endocrinol Metab 2007;92:3875-3884
Copyright ©2007 The Endocrine Society
35
(μg/dl)
Cortisol
Cortisol (μg/dl)
30
25
20
20μg/dl
15
10
5μg/dl5
0
1
2
3
4
5
6
7
8
9
10
11
12
13
Pros and Cons of GH Treatment During the Transition
Period
•Window of opportunity exists – therefore interruption of therapy for prolonged
period of time (years) potentially disadvantageous.
Improves
• Bone mineral content
• Body composition
• Muscle development and strenght
• Lipid profils
• Cariovascular function
No discernible effect on
• Quality of life
Possible negative effect on
• Insulin sensitivity
Dosing questions: How much? And should females receive higher doses?
Tasks after The Diagnosis
• Start with low dose (0.2-0.5 mg/day) and adjust the
dose according to IGF-I concentrations.
Monitor:
• IGF-I
• BMD and body composition
• Glucose and lipid
metabolism
• Thyroid and adrenal
function
••How
QOL
to handle metabolic parameters in daily practice?
• Evolving pituitary defects
Summary -1
• Patients with high likelihood of permanent GHD and their
families should be educated that GH treatment may be lifelong.
Testing for GH deficiency should be undertaken with an
intention to treat in patients at risk of permanent GHD
• ITT is a reliable test during the transition period and
biochemical GH deficiency could be actually defined by a peak
GH response of < 6 µg/L
• Patients with CRT-induced GHD yielded false positive
responses to GHRH plus Arginine within the first 10 years after
irradiation
• Assay standardization remains an important unresolved issue.
Universally adopted calibrators for GH and IGF-I assays are
required. The availability of age specific normative data for IGFI assays would be highly advantageous to clinical management.
Summary -2
• Treat with GH starting with low dose and adjust
according to IGF-I levels. Monitor for efficacy and
side-effects
• Patients’ quality of life desires should be taken into
account
• Interaction between the pediatric and the adult
endocrinologist with experience in treating adult
GHD is essential to provide continuity of care
• Provide a smooth transfer of care from the pediatric
to the adult endocrinologist with experience in
treating GHD
Acknowledgments
Cagliari
Sandro Loche
Bambino Gesù
Marco Cappa
Bolzano
Giorgio Radetti
Napoli
Maria Carolina Salerno
Torino
Lucia Ghizzoni
Pediatric Endocrinology
Natascia Di Iorgi
Flavia Napoli
Anna Allegri
Annalisa Calcagno
Roberto Gastaldi
Neuroradiology
Andrea Rossi
Gionanni Morana
MariaSavina Severino
Staff Nurses
Patrizia Salusciev
Graziella Ferrieri
Maria Aulicino
Gloria Piras
Patients and Families
 [PDF")