XVI Congresso nazionale SIGU - Corso post congressuale
Eterogeneità genetica nei tumori ereditari:
quali test proporre nella pratica clinica
Percorso diagnostico delle
POLIPOSI ADENOMATOSE
e AMARTOMATOSE
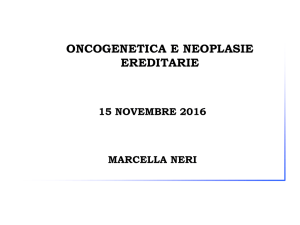
Familial CRC
~ 15%
Hereditary CRC
~ 3%
~ 1%
Non-polyposis
“Polyposis”
FAP ; AFAP
MAP
Sporadic CRC
1: >10.000
Peutz-Jeghers
1: <100.000
Juvenile Polyposis
Hereditary Mixed Polyposis
Cowden Syndrome
NEW
2013!
Polymerase
proofreading-associated
polyposis (PPAP)
As yet undiscovered
? Hereditary Colo-Rectal Cancer
“Polyposis”
Non-polyposis
ADENOMA -> CARCINOMA
5 - 10 years
3 - 5 years
Hyperproliferation
Normal
Adenoma: Adenoma: Adenoma: Cancer: Cancer:
early
intermediate late
“curable” late
Only ~ 25% adenomas progress to cancer
POLIPI IPERPLASTICI
POLIPI AMARTOMATOSI
POLIPI INFIAMMATORI
….
? Hereditary Colo-Rectal Cancer
“Polyposis”
> 1000
Non-polyposis
0
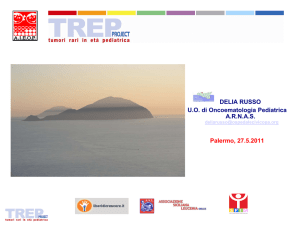
Prevalenza di adenomi, adenomi avanzati e cancro in
programmi di screening endoscopico
Adenomi
AD Avanzati
Cancro
Rettosigmoidoscopia
UKFSS-Trial 2002 (55-64 yrs)
12%
5%
0.04%*
SCORE I 2002
(55-64 yrs)
11%
3%
0.05%*
IST 2008
(55-64 yrs)
13.5%
3%
0.05%
(50 yrs)
37%
10%
1.0%
Regula 2006
(50-66 yrs)
14%
6%
0.9%
IST 2008
(55-64 yrs)
26%
8%
1.1%
Colonscopia
Lieberman 2000
* Rimozione endoscopica: UKFFS: 17% (17/140)
SCORE-I: 20% (11/54)
QUANTI (e quali) POLIPI fanno una ‘POLIPOSI’ ??
- iperplastici
- adenomatosi
- amartomatosi (vari sottotipi)
Histology
Syndrome
Gene
Adenomatous
polyposis
FAP ; AFAP
APC
MAP
MUTYH
Peutz-Jeghers
Juvenile Polyposis
Cowden Syndrome
(BRRS; Proteus s.)
STK11/LKB1
SMAD4; BMPR1A
PTEN
Hyperplastic
polyposis
Hamartomatous
Polyposis
POLIPOSI ADENOMATOSE
Poliposi Familiare Adenomatosa (FAP)
classica
•
•
•
Malattia rara: 1: 11.000 – 1: 37.000 (European Medicine Agency)
descritta già nel 1700 e 1800
Lockhard-Mummery (1925): rischio di CRC
•
•
•
•
Autosomica dominante ad alta penetranza
20-30% non c’è famigliarità ( ‘de novo’ )
1987 Linkage 5q21 (no evidenza di eter.gen.)
1991 clonaggio posizionale gene APC
•
Centinaia-migliaia di adenomi colorettali
•
•
•
•
Eta’ media insorgenza: 16-25 anni*
Eta’ media diagnosi: 36 anni*
Eta’ media cancro: 34-43 anni*
Rischio di cancro colorettale 100%
*serie storiche prima dell’endoscopia
•
S. Gardner (1953)
– manifestazioni colorettali ed extra come FAP
– desmoidi (8-13%)
– osteomi cranio e ossa lunghe
– alterazioni dentarie
– cisti sebacee ed epidermoidi
– lipomi, fibromi
– neoplasie del surrene e vie biliari
•
S. di Turcot (1959)
– piu’ rara della S.di Gardner
– manifestazioni colorettali (ed extra) come FAP
– neoplasie cerebrali
• gene APC (medulloblastoma)
• geni MMR (glioblastoma multiforme)
(eterogeneità genetica)
DIAGNOSI
“ PERSONS WITH MORE THAN
100 COLORECTAL ADENOMAS
HAVE FAP BY DEFINITION ”
American Association
of Gastroenterology, 2003
• FAP attenuata
(AAPC o AFAP) (1990)
–
–
–
–
–
adenomi colorettali multipli ( < 100 )
alta variabilita’ intra-familiare n. adenomi
localizzazione piu’ frequente a destra
alto rischio di cancro colorettale
eta’ di insorgenza piu’ avanzata
quanti adenomi fanno una ‘FAP’??
CLASSIFICATION OF FAP:
A DIAGNOSTIC NIGHTMARE
Lynch, Am J Hum Genet 1998
FAP
N.
adenomi
Poliposi profusa
Poliposi classica
AFAP
Poliposi sparsa
sporadici Poliposi attenuata
Poliposi molto attenuata
10 – 99 adenomi
Al Tassan et al., Nature Genetics Feb. 2002
“Multiple adenoma” CRC Family
*
*
*
APC Germline:
* E1317Q
APC Somatic:
15 of 18 G:C -> T:A transversions
MUTYH-Associated Polyposis (MAP)
autosomal recessive adenomatous polyposis
gene mutato
MUTYH – Associated Polyposis (MAP)
Adenomas
“polyposis”
somatic APC
Hyperplastic/ serrated polyps
(>40%)
“CRC without polyposis”
K-ras
CRC : MSI-L
42% only 1 syncronous polyp at CRC diagnosis
(Croitoru et al, JNCI 2004)
35% no polyp at CRC diagnosis
(Cleary et al, Gastroent 2009)
276 MAP pts
Muir-Torre
No desmoids
No osteomas; CHRPE rare
Gastric polyps 11%
Duodenal
adenomas
17%
HNPCC
…. Diagnosi molecolare
FAP (Familial Adenomatous Polyposis)
vs
MAP (MYH-ASSOCIATED POLYPOSIS)
90%
(DOMINANTE)
10%
Profuse
Classic
> 100
Sparse
Attenuated < 100
Multiple
CRC 40 anni
(RECESSIVO)
? < 20
CRC 50 anni
Hyperplastic polyposis
Hyperplastic polyposis syndrome (HPS)
May be heterogeneous
It may have two phenotypes:
(1) the presence of at least 30 (but not necessarily large) hyperplastic polyps in a
pancolonic distribution,
(2) five hyperplastic polyps proximal to the sigmoid colon with at least two being 1
cm in diameter or larger
Some examples can meet both definitions.
The proximal and large polyps occurring in the second type of hyperplastic
polyposis are likely to be sessile serrated adenomas (SSAs).
Molecular research in SSAs strongly suggests that these polyps are precursor
lesions that may lead to CRC (BRAF, MSI-H).
Conceivably, the risks of cancer and the molecular pathway of carcinogenesis may
differ, with MSI-H cancers linked more closely to the second category.
More research is required into the phenotypic and genotypic diversity of
hyperplastic polyposis
Genetic predisposition ?
Hamartomatous polyposis
Peutz-Jeghers Syndrome
= association of gastrointestinal polyposis and mucocutaneous pigmentation
PJ hamartomatous polyps* most common in the small intestine
(in order of prevalence: in the jejenum, ileum, and duodenum)
but can also occur in the stomach and large bowel
* histopathologically: unique finding of mucosa with interdigitating smooth muscle bundles
in a characteristic branching tree appearance
Adenomas also appear with increased prevalence throughout the gastrointestinal tract
chronic bleeding and anemia
recurrent obstruction and intussusception requiring
repeated laparotomies and bowel resections
Age at onset (symptoms) is variable :
Laparotomy for bowel obstruction :
- median age 10 years
- some within the first few years of life
30% by age 10 years
68% by age 18 years
Juvenile Polyposis Syndrome (JPS)
predisposition to hamartomatous polyps in the gastrointestinal (GI) tract,
specifically in the stomach, small intestine, colon, and rectum
The term "juvenile" refers to the type of polyp* rather than to the age of onset of polyps
Most individuals with JPS have some polyps by age 20 years
Number of polyps: from 4-5 polyps to > 100 over their lifetime
If the polyps are left untreated, they may cause bleeding and anemia.
Most juvenile polyps are benign; however, malignant transformation can occur
Risk of GI cancers in families with JPS ranges from 9% to 50%.
Most of this increased risk is attributed to colon cancer,
but cancers of the stomach, upper GI tract, and pancreas have been reported.
* hamartomas that develop from an abnormal collection of tissue elements normally present at this site:
Juvenile polyps show a normal epithelium with a dense stroma, an inflammatory infiltrate, and a smooth
surface with dilated, mucus-filled cystic glands in the lamina propria. Muscle fibers and the proliferative
characteristics of adenomas are typically not seen in juvenile polyps.
Juvenile Polyposis Syndrome (JPS)
Two genes are known to be associated with JPS:
BMPR1A. ~20% [Sayed et al 2002, Howe et al 2004].
SMAD4. ~ 20% [Howe et al 2004].
Genotype-phenotype correlations in general are poor
- some members of families with JPS and the same mutation have a few polyps,
whereas others have more than 100;
- the age at which polyps develop can vary from the first decade to beyond
the fourth decade among affected members of the same family
• SMAD4 more likely to have a family history of upper-GI polyps
• SMAD4 or BMPR1A more likely to have more than ten lower GI polyps
and a family history of GI cancer [Burger et al 2002, Friedl et al 2002, Sayed et al 2002].
PTEN Hamartoma Tumor Syndrome (PHTS)
[Includes: Cowden Syndrome, Bannayan-Ruvalcaba-Riley Syndrome
(Bannayan-Riley-Ruvalcaba Syndrome, Bannayan-Zonana Syndrome,
Riley-Smith Syndrome, Ruvalcaba-Myhre-Smith Syndrome), Proteus Syndrome]
Major criteria
Breast cancer
Epithelial thyroid cancer (non-medullary), especially follicular thyroid
cancer
Macrocephaly (occipital frontal circumference ≥ 97th percentile)
Endometrial carcinoma
Minor criteria
Other thyroid lesions (e.g., adenoma, multinodular goiter)
Mental retardation (IQ ≤ 75)
Hamartomatous intestinal polyps*
Fibrocystic disease of the breast
Lipomas
Fibromas
Genitourinary tumors (especially renal cell carcinoma)
Genitourinary malformation
Uterine fibroids
Cancer Risk
25%-50%
~10%
5%-10%
CRC risk not increased
* PHTS hamartomatous polyps are different in histomorphology from
the polyps seen in Peutz Jeghers syndrome
…la realtà non è fatta (solo) di situazioni da manuale….
Famigliarità
comune
AFAP
HNPCC
FAP
Altre poliposi
CRITERI CLINICI
DETECTION RATE
“Polyposis”
adenomi
Non-polyposis
polipi
amartomi
iperplastici
Documentazione istologica
completa !!
- numero delle lesioni
- biopsie non sono rappresentative
- non concordanza tra patologi
quadri «misti»
……in alcuni casi
revisione istologica da parte
di un patologo esperto
DD tra poliposi amartomatose per invio
al (primo) test genetico
“Polyposis”
Non-polyposis
amartomi
Fenotipo ?
1. Storia personale: altri segni clinici /patologie
2. Storia famigliare: suggestiva?
3. Revisione istologica (patologo esperto!!)
Expertise personale ?
(rare e molto rare!!)
(RETE) MALATTIE RARE
Consulenza
Genetica
Multidisciplinare
in Centro
Esperto
DD tra FAP e MAP per invio al (primo) test genetico
“Polyposis”
Non-polyposis
adenomi
Modello ereditarietà ?
1. Verticalità
2. In assenza di verticalità, FH in fratelli/sorelle
3. In casi singoli, consanguineità (nota o presumibile)
Fenotipo ?
1. Età diagnosi
2. Numerosità degli adenomi
3. Desmoide
4. Polipi iperplastici/serrati
Utilità del test ?
1. Fratelli/sorelle
2. Figli
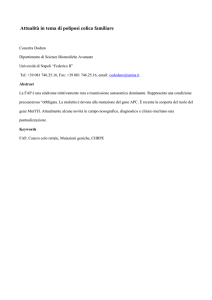
DD tra FAP e MAP per invio al (primo) test genetico
“Polyposis”
Non-polyposis
adenomi
>100 ad
Verticalità
<40 anni
<100 ad
Solo fratria / consanguineità
>50 anni
Test APC
Test MUTYH
Test APC & MUTYH
Altri test??
MSI
STK11..
POLYMERASE PROOFREADING-ASSOCIATED POLYPOSIS
(PPAP)
NEW
2013!
SM7
WGS in 3 members
Previous linkage data from 5 individuals with > early-onset colorectal adenomas
8 shared regions of the genome
WGS: 6 non-silent variants in 4 regions shared by the 3 individuals
Genotyping in additional affected showed that only shared one of these:
POLE c. 1270C>G (p.Leu424Val)
POLE
Validation set
12
0
Casi
3.805 individuals European ancestry with CRC,
enriched for family history of CRC,
multiple adenomas and early-onset disease
Controlli
6.721 individuals European ancestry,
2/3 population-based and 1/3 selected for
absent personal history of colorectal tumors
3 ogni 1.000 CRC «enriched»
- Dominant inherited trait (highly penetrant)*
- All (except one) pedigrees at least 1 individual with:
multiple or very large adenomas,
multiple CRC or early-onset CRC
POLE
Affected status:
- > 5 colorectal adenomas
- > 1 large (>2 cm in diameter) adenoma
- >2 colorectal carcinomas
- < 40 years of age at diagnosis of CRC
SM6
Previous linkage
shared regions of the genome
WGS: variants shared
by the individuals
(common ancestor)
SM4
POLD1 c. 1433G>A
(p.Ser478ASn)
POLD1
Validation set
1
0
Casi
3.805 individuals European ancestry with CRC,
enriched for family history of CRC,
multiple adenomas and early-onset disease
Controlli
6.721 individuals European ancestry,
2/3 population-based and 1/3 selected for
absent personal history of colorectal tumors
1 ogni circa 4.000 CRC «enriched»
- Dominant inherited trait
- Endometrial cancer
- Brain tumors
POLE L424V and POLD1 S478N variants can be easily tested for and
should be considered in any individual with an unexplaned
personal or family history of
- multiple or large colorectal adenomas and/or
- multiple or early-onset colorectal (or endometrial) carcinoma.
“Le evidenze sui benefici dei nuovi test genetici sono spesso deboli”
Alti livelli di evidenza di utilità clinica
anni senza poter applicare in clinica
le scoperte sui geni/genoma +
ricerca e sviluppo nel settore
fortemente disincentivati
Livelli di evidenza
non definiti/ molto bassi
potenziale rischio di effetti dannosi per
gli utenti/pazienti e i sistemi sanitari
“evidence dilemma”
Public Health Genomics (PHGen)
CONOSCENZA
MONDO POLITICO
(decisori)
Informazioni per scegliere
(multidimensionali, multidisciplinari)
metodologia HTA
(Health Technology Assessment)
Aree: - tecnologia
- paziente (etico-sciale)
- economia
- organizzazione