Sorveglianza Internazionale delle
Paralisi Flaccide Acute
Lucia Fiore
CRIVIB
Istituto Superiore di Sanità
Workshop
SORVEGLIANZA
DELLE PARALISI FLACCIDE ACUTE
E DELL’INFEZIONE DA ROTAVIRUS IN ITALIA
Roma, 15-16 Marzo 2012
Poliomielite Malattia Antica
Grave malattia infettiva a carico
del sistema nervoso centrale,
colpisce i motoneuroni delle corna
anteriori del midollo spinale e si
manifesta con una paralisi flaccida.
Nota già nell’antico Egitto
(XVIII dinastia, 1400 a.C.)
e nella Grecia classica è stata
endemica per migliaia di anni.
Prime segnalazioni di epidemie da
trasmissione indiretta e da contagio
interumano, inizio e fine dell’ottocento.
Poliomielite
L’età colpita è soprattutto la prima infanzia
ma in passato interessava anche gli adulti
Philip Roth
Nel quartiere ebraico di Newark, - il luogo, appunto, dell‘"origine", dove vive gente normale e modesta
come poche, nel luglio 1944 scoppia un'epidemia di poliomielite, che miete vittime e lascia terribili
strascichi, com'è ovvio, soprattutto fra i bambini.
Roth ci guida fra le più piccole sfaccettature di ogni emozione che una simile epidemia può far scaturire:
paura, panico, rabbia, confusione, sofferenza e dolore. L'epidemia di polio, è imprevedibile e inafferrabile.
1955 Il vaccino inattivato di Salk
1953 Vaccino attenuato di Sabin
Qual é la differenza tra i due tipi di vaccino?
Il vaccino Sabin (OPV), é un vaccino vivo attenuato.
Essendo somministrato oralmente, stimola sia l’immunità intestinale
(con produzione e rilascio di anticorpi secretori, (IgA) che l’immunità
umorale (produzione di anticorpi nel sangue, prevalentemente IgG).
Il vaccino Salk (IPV), è un vaccino inattivato e produce una più che
soddisfacente immunità umorale in grado di garantire la protezione del
soggetto immunizzato ma non è in grado di indurre una efficiente
risposta immunitaria a livello intestinale (IgA secretorie).
Quali sono gli effetti collaterali dei due vaccini?
Il vaccino inattivato di Salk non ha praticamente effetti collaterali
Il vaccino Sabin ha effetti collaterali: rischio di poliomielite associata a
vaccinazione (VAPP), molto basso 1 caso per 600.000 - 1.000.000 bambini
vaccinati con la prima dose e 1 caso su 12.000.000 di bambini vaccinati con
le dosi successive. Causati in particolare dai sierotipi 2 e 3 che sono
geneticamente più instabili.
Come avviene il contagio della malattia polio ?
• Per via oro-fecale
• Il poliovirus si moltiplica nella mucosa oro-faringea,
nell’intestino e nei tessuti linfatici sottostanti
• Dopo la fase viremica il virus può raggiungere il
sistema nervoso centrale, replicarsi nei neuroni
motori e provocare la paralisi.
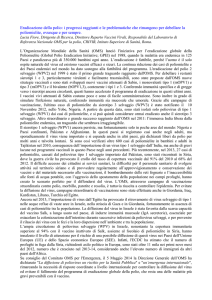
• Su 100-200 soggetti infetti, mediamente uno solo si
ammala.
PARALYTIC
AFP SURVEILLANCE raises
the “iceberg”
NON-PARALYTIC
New Infections
“Reinfections”
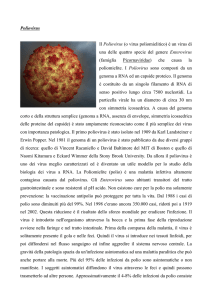
I poliovirus
Gli agenti eziologici della poliomielite sono i
tre sierotipi (1, 2 e 3) di poliovirus, appartenenti
al genere enterovirus.
I poliovirus sono virus ad RNA a singolo
filamento, a polarità positiva circondati
da un capside icosaedrico.
Struttura tridimensionale del Poliovirus
La poliomielite si può eradicare perché:
• Esistono vaccini efficaci
• L’uomo è l’unico reservoir in natura
Polio nel 1988
125 paesi endemici
> 500.000 casi anno
1988: World Health Assembly Resolution
Strategie per l’eradicazione della polio
1. Routine Immunization
2. National Immunization
Days (NIDs/SNIDs)
3. Surveillance AFP &
Environment
4. Mop-ups
Paralisi Flaccide Acute (AFP): Gold Standard
Ambientale dei liquami (WHO Guidelines)
Attività supplementare
Enterovirus (principalmente meningite asettica)
Alternativa all’ AFP/ Attività supplementare
(WHO Guidelines 2011)
Definizione di AFP
Sindrome ad inizio rapido ed improvviso caratterizzata da paresi o paralisi degli arti.
Nei casi più gravi vengono coinvolti anche i muscoli respiratori o della deglutizione.
Il termine flaccido indica l’assenza di spasticità dei muscoli colpiti nonché l’assenza di altri
segni come ipereflessia, cloni, riflesso plantare di estensione.
Possibili cause di AFP
Poliomielite
Paralisi similpoliomielitica (causata da altri enterovirus)
Guillan-Barré
Mielite trasversa
Mielite traumatica
Paralisi da tumore (se non diagnosticata immediatamente)
Indicatori di qualità della sorveglianza delle AFP
Tasso AFP-non polio in soggetti tra 0-15 anni
Obiettivo 1 / 100,000
Completezza: % di tutte le notifiche settimanali di AFP ricevute
Obiettivo: 90%
Tempestività: % di tutte le notifiche attese ricevute entro i termini
Obiettivo: 90%
Indagine 48 ore dalla segnalazione
Obiettivo: 80%
2 campioni di feci 24 ore di distanza e 14 giorni inizio paralisi
Obiettivo: 80%
Follow-up del paziente entro 60 giorni per verifica paralisi residue
Obiettivo: 80%
Global Laboratory Network for Polio Eradication (1991-2011)
Specialised Reference Laboratory
Regional Reference Laboratory
National/ Sub-national Laboratory
The designation employed and the presentation of material on this map do not imply the expression of any opinion whatsoever on the part of the secretariat of the World Health Organisation concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
OMS polio LabNet:
•
•
•
•
•
Protocolli standard
Linee cellulari e reagenti standard
Indicatori standard di performance
Strumentazione adeguata
Laboratory Data Management System (LDMS) “Data base” per
l’inserimento dei dati epidemiologici e di laboratorio nazionali e regionali.
ACCREDITAMENTO
•
•
•
•
Corsi di formazione
Check-list annuale
Visite ispettive
PTS annuale
17th Informal Consultation on the
Global Polio Laboratory Network
WHO Geneva
21-23 September 2011
Sorveglianza delle AFP nella Regione
Europea dell’OMS
Polio LabNet OMS/Europa
52 Stati Membri
Network di 48 laboratori in 37 paesi
7 laboratori specializzati
-
Lab
Nazionali
accreditati
Senza Lab
Nazionali
Lab RRL/Specializzati
Sorveglianza dei Poliovirus nella Regione Europea dell’OMS
Ambientale
Sorveglianza AFP
Sorveglianza AFP più altre
Sorveglianza Enterovirus
Paesi afferenti al Laboratorio Regionale di
Referenza di Roma (ISS)
ISS
Con laboratorio nazionale
(Serbia,Montenegro, Grecia,
Bulgaria, Albania, Macedonia)
Senza laboratorio nazionale
(Kosovo, Bosnia, Malta)
Poliomielite nella Regione OMS-Europa
Epidemia in Albania (1996)
140 soggetti colpiti di cui 16 morti
(poliovirus tipo 1 selvaggio importato dal Pakistan)
Diamanti E et al. Vaccine (1998) 16: 940-947.
Prevots D.R, et al Clin. Inf. Dis. (1998) 26: 419-25.
Fiore L. et al. J. Clin. Microbiol. (1998) 36: 1912-8.
Marturano J. & Fiore L. J. Clin. Microbiol. (2002), 40: 316-317.
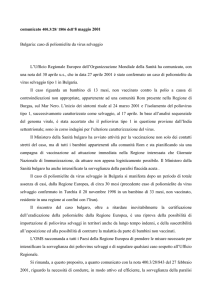
Casi di poliomielite in Bulgaria 2001
3 CASI
2 CONTATTI
Bambini nomadi
non vaccinati
Kunchev, M. et al MMWR (2001), 50 (46):1033-5.
Kojouharova M., et al. 2001. (2003) WHO Bulletin 81, 1-7.
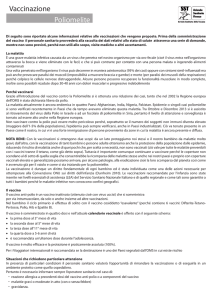
Correlazione genetica tra polio selvaggi importati in Bulgaria
(2001) e Georgia (2001) e virus circolanti in India
7TAJ91
CHN99C
98
CHN99
2000022715
60342SYR
100
69
2000022678
100
UPMRD00018
100
306BUL01
100
478BUL01
61
99
239BUL01
100
378BUL01
2000022688
95
2000022677
99
2000022718
87
99010388
7299010391
99010428
0.01
Non-polio AFP Rate
Nov 2009 – Oct 2010
Nov 2010 – Oct 2011
< 0.5
0.5 - 0.99
>1
No AFP Surveillance/data
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of
the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the
delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full
agreement.
@ WHO 2011. All rights reserved
Data in WHO/HQ as of 06 Dec 2011
Adequate Stool Collection Rate
Nov 2009 – Oct 2010
Nov 2010 – Oct 2011
< 60%
60% - 79.99%
> 80%
No AFP Surveillance/data
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of
the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the
delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full
agreement.
@ WHO 2011. All rights reserved
Data in WHO/HQ as of 06 Dec 2011
Surveillance indicators, polio endemic regions
Nov 2010 – Oct 2011
Non-polio AFP rate
<1
1 – 1.99
>= 2
Adequate stool collection rate
< 50%
50 – 79.99%
>= 80%
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of
the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the
delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full
agreement.
@ WHO 2011. All rights reserved
Data in WHO/HQ as of 06 Dec 2011
Sub-national Non Polio AFP rate
May – Oct 2011
<1
1 – 1.99
>= 2
Areas with population
under 15 yrs <100,000
Only WPV endemic, re-established, and WPV importation belt countries are mapped.
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever
on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities,
or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which
there may not yet be full agreement.
@ WHO 2011. All rights reserved
Data in WHO/HQ as of 06 Dec 2011
Sub-national Stool Adequacy rate
May – Oct 2011
< 50%
50 – 79.99%
>= 80%
Areas with population
under 15 yrs <100,000
Only WPV endemic, re-established, and WPV importation belt countries are mapped.
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever
on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities,
or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which
there may not yet be full agreement.
@ WHO 2011. All rights reserved
Data in WHO/HQ as of 06 Dec 2011
GPLN performance
GPLN workload
No. specimens & WPV by source, 2009 to 2011 (to June)
250000
200000
150000
"Not WPV"
WPV
100000
50000
0
"Not WPV"
WPV
2009 AFP
2009 Non-AFP
2010 AFP
2010 Non-AFP
2011 AFP
2011 Non-AFP
176005
15055
191997
17287
91837
8672
2963
160
1649
151
818
78
Total of 211,084 samples from all sources analysed in 2010
Approximately 1.0 % of all specimens yielded WPV
91.7 % workload from AFP and 8.3% from non-AFP sources
% Virus Isolation Resullts reported on time, by Region
2008 to 2011 (to June)
120
100
80
2008
2009
60
40
20
0
2010
2011
AFR
AMR
EMR
EUR
SEAR
WPR
% NPEV isolation rate
by Region
25
20
2008
15
2009
2010
10
2011
5
0
AFR
AMR
% ITD results within 60 days of AFP onset
2009 to 2011 (to June)
120
100
80
2009
60
2010
2011
40
20
0
AFR
AMR
EMR
EUR
SEAR
WPR
EMR
EUR
SEAR
WPR
Global Polio Laboratory Network Accreditation Status
(data as of September 2011)
Year
Fully
Accredited
Provisionally
Accredited
2008
136
6
1
1
144
95.1
2009
134
5
2
3
144
95.0
2010
139
2
0
5
146
98.6
2011
137
5b
0
4c
146
96.5
a. Labs pending accreditation are excluded
b. KEN, CAR, MEX, KUW, SPA (Spain)
c. VEN, BRA (Bélem), CAN, UZB.
Failed Pending Total
% fully
accredited a
Polio Laboratory Accreditation Status by Region
(data as of September 2011)
Region
Fully
accredited
Provisionally
accredited
AFR
14
2
AMR
7
1
EMR
11
1
EUR
46
1
SEAR
16
WPR
TOTAL
*
a.
b.
c.
d.
Not
accredited
Pending
Total
% fully accredited
( % in 2010) *
a
0
0
16
87.5 (100)
b
0
3
11
87.5 (77.7)
c
0
0
12
91.6 (91.6)
d
0
1
48
97.8 (97.9)
0
0
0
16
100 (100)
43
0
0
0
43
100 (100)
137
5
0
4
146
96.5 (98.6)
Labs pending accreditation are excluded
KEN (Nov-10) and CAR (May-11); both succeeded virus isolation and rRT-PCR PT
MEX (succeeded in virus isolation PT)
KUW (succeeded in rRT-PCR PT)
SPA (Spain, problems with virus isolation PT))
Proficiency test for sequencing
Proficiency test started in 2011
Using same panel of specimens as rRT-PCR PT
No score to be assigned in 2011, but qualitative feedback to
be provided.
Evaluation of Consensus Protocol
for use of FTA Cards
• GPLN laboratories in certain countries are unable
to ship infectious materials for ITD/sequencing
due to national regulations
• Specimens from these areas are key to the
Programme due to risk of polio transmission and
adjacency to endemic countries
• Evaluate Whatman FTA Cards as a means to
inactivate virus and facilitate shipping
Proficiency test for Cell sensitivity
Authentication of cell lines used for poliovirus isolation
L20B Cell Sensitivity Testing 2003-2010
9,5
Polio 1
Polio 2
Polio 3
9
8,5
8
7,5
Javier Martín
NIBSC UK
Biosafety Training Materials
Polio: Ultimi Casi nelle Regioni polio-free
Americas Region
Luis Fermin Tenorio
Peru 1991
Western Pacific
Region
Mum Chanty
Cambodia 1997
European Region
Melik Minas
Turkey 1998
Polio Eradication
Poliovirus di tipo 2 selvaggio eradicato nel 1999!!!
Diffusione dei Poliovirus in Paesi polio-free (2003-2008)
2005
2193 casi
Tipo 1
Tipo 3
Paesi endemici
Importazione in corso
Outbreak bloccati nel 2007
Data in HQ as of 09 October 2006
100 importazioni di virus selvaggi, 2003-2008
circa 700 casi di poliomielite in Nigeria
Rischio Gap Immunizzazione
Human consequences
Number of cases in polio outbreak countries
2003-2009*
Number of cases
1200
cVDPV cases
Total: 2193 cases
WPV cases
1000
800
600
400
200
0
2003
2004
2005
2006
2007
2008
2009*
Financial consequences
External funds spent on outbreak control 2003 -2009
*Data in HQ as of 27 May 2009
Millions US $
250
Op Costs
Total: US$ 857 Millions
Vaccine
200
150
100
50
0
2003
2004
2005
2006
2007
2008
2009
Data in HQ as of 03 June 2009
Wild Poliovirus*, 10 March 2009 – 09 March 2010
2009: 1604 cases (1256 in E.C.)
479 type 1 e 1174 type 3
Wild virus type 1
Wild virus type 3
Wild virus type 1/3
Endemic countries
Case or outbreak following importation (0 - 6 months)
Case or outbreak following importation (6 - 12 months)
prevalente
il sierotipo 3
*Excludes viruses detected from environmental
surveillance and vaccine derived polioviruses
Wild Poliovirus, 29 Dec 2009 – 28 Dec 2010
prevalente
il sierotipo 1
Wild virus type 1
Wild virus type 3
Wild virus type 1/3
Endemic countries
Case or outbreak following importation (0 - 6 months)
Case or outbreak following importation (6 - 12 months)
2010 - 1292 cases
449 in WHO Europe:
435 Tajikistan & 14 Russian Federation)
450 in Congo
, 87 type 3
Importazione di un ceppo PV1 selvaggio dall’India
A new poliovirus entered the country
600 bambini e giovani adulti
paralizzati!
Una risposta imponente !
• Oltre 15 milioni di vaccinazioni polio effettuate
in Tajikistan nel 2010
• Una grande copertura di tutta la popolazione
sotto I 25 anni !
• Il Rotary ha fornito un milione di dollari per
l’acquisto di vaccini !
• Un successo reale: da più di un anno nessun
altro caso, nè virus circolanti !
Detection of imported WPV1 in China 2011
Country
China
China
China
China
Epid-no
DONSET
15116 19-Jul-11
15115 17-Jul-11
15117 11-Jul-11
15114 03-Jul-11
Type
W1
W1
W1
W1
Province
Xinjiang
Xinjiang
Xinjiang
Xinjiang
District
Hetian (or Hotan)
Hetian (or Hotan)
Hetian (or Hotan)
Hetian (or Hotan)
Luglio - settembre 2011
22 casi e un morto
nello Xinjiang
al confine con il Pakistan
Virus imported from Pakistan
• Lab confirms China outbreak within 7 days
of receipt of isolate for ITD and within
28 days of the onset of the first case.
• Likely link to Pakistan & not Tajikistan
2010 as shown in dendrogram prepared by
RRL China.
• Link confirmed by CDC-USA within 2.5
hours of receipt of Dr. Wenbo's message.
• Complete comparison to all Afghanistan &
Pakistan viruses & summary dendrogram
provided by Pakistan lab within 24 hours
of request.
Detection of SOAS WPV1 importation in China
4 milioni e mezzo di
bambini e giovani
sono stati vaccinati
contro la polio nello
Xinjiang
• RRL-China confirms China outbreak within 7 days of receipt
of isolate for ITD and within 28 days of the onset of
the first case.
• Likely link to Pakistan & not Tajikistan 2010 outbreak
shown in dendrogram prepared by Dr. Wenbo.
• Link confirmed by CDC-USA within 2.5 hours of
receipt of Dr. Wenbo's message.
• Complete comparison to all Afghanistan &
Pakistan viruses & summary dendrogram
provided by Pakistan lab within 24 hours of request.
Wild Poliovirus1, Febbraio 2011 – Febbraio 2012
2012
L’OMS ha rimosso
l’INDIA dai paesi polio
endemici !!!
Wild virus type 1
Wild virus type 3
Wild virus type 1/3
L’ultimo caso indiano
è del 13 Gennaio 2011!!!
Endemic country
Country with WPV case in previous 6 months
1Excludes
viruses detected from environmental surveillance and vaccine
derived polioviruses.
Data in WHO HQ as of 06 Mar 2012
Vaccinazione anti-polio:
NID, esperienza dei volontari Rotary italiani in
India
Wild Poliovirus1, 30 Nov 2011 – 29 May 2012
2012 Gennaio-Maggio
Minor numero casi
polio nel mondo,
nella storia!!
Wild virus type 1
Wild virus type 3
Wild virus type 1/3
Solo 64 casi
Endemic country
Country with WPV case in previous 6 months
1Excludes
viruses detected from environmental surveillance and vaccine derived
polioviruses.
Data in WHO HQ as of 29 May 2012
Attività intraprese per interrompere la
trasmissione dei poliovirus selvaggi
Nuove Strategie per la vaccinazione
(2005-2010)
Produzione di Vaccini Monovalenti tipo 1 e 3
somministrazione come prima dose o booster
in Africa e India
tOPV
MOPV1
MOPV3
Uso del vaccino monovalente OPV tipo 1
(mOPV1) 2006-2007
mOPV1 trials clinici
Egitto, 2006
mOPV1
2006-2007 (N = 24 Paesi)
75
50
% children protected
against type1
after birth dose
25
0
'trivalent' OPV
'new' mOPV1
2.4 miliardi dosi
2006-2007
Data in WHO HQ as of 19 June 07
Uso del vaccino monovalente OPV tipo3
(mOPV3) 2007-2008
Paesi che hanno usato mOPV3
mOPV3
Data in WHO HQ as of 1 Oct 07
75 milioni di dosi
2007-2008
Nuove Strategie
(2005-2009)
Produzione di vaccini monovalenti tipo1 e 3
somministrazione come prima dose o booster
in Africa e India
Nuove Strategie per la Vaccinazione
(2010-2011)
Produzione di Vaccini Bivalenti (Polio1 e polio3)
bivalent
OPV
Efficacia del vaccino Bivalente OPV & uso
Seroconversion after 2 x bOPV
vs. tOPV, India, 2008-2009
bivalent OPV use
as of Sept 2011
100
90
80
79,5
71
70
60
53,2
49,1
50
40
30
20
10
Introduced
Dec 09-Aug 11
0
bOPV
tOPV
bOPV
tOPV
Planned by
end-2011
Type 1
Type 3
67
Immissione in commercio del bOPV & uso 2009-2011
bOPV products licensed and pre-qualified.
Panacea
India
Year
Grand
Total
GSK
Belgium
bOPV
Bio Farma
Indonesia
Haffkine
India
Bharat
India
Sanofi Novartis
Pasteur
Italy
France
mOPV1
mOPV3
tOPV
Grand Total
2005
466,366,142
8,433,735
1,728,478,957
2,203,278,834
2006
985,935,841
7,504,245
1,225,058,449
2,218,498,535
2007
1,203,333,392
196,465,452
1,067,430,981
2,467,229,825
2008
1,123,468,862
383,664,620
874,483,393
2,381,616,875
2009
3,493,794
1,098,596,271
206,671,909
918,204,766
2,226,966,740
2010
888,781,302
502,870,471
80,150,724
730,646,977
2,202,449,474
892,275,096
5,380,570,979
882,890,685
6,544,303,523
13,700,040,283
Not included above, ~700 million doses of tOPV per year for routine immunization
69
Altre Emergenze
Casi VAPP
Casi di paralisi associata a vaccino
riceventi o contatti
500 per anno in tutto il mondo!!
Epidemie causate da
Poliovirus derivati da Vaccino (cVDPV)
Virus derivati dai ceppi Sabin che hanno accumulato mutazioni in
diverse regioni del genoma
Paradosso
Wild
PV2 eradicato
Circulating Vaccine-derived Poliovirus from AFP cases, 2000-2011
Country
Mozambique
Myanmar
Indonesia
China
Philippines
DOR/Haiti
Country
2000
2002
2003
2007
1
4
2008
2009
2010
2011
2
46
2
12
2000
Nigeria
Yemen
Somalia
Afghanistan
Chad
DRCongo
Niger
India
Ethiopia
Madagascar
Country
2001
cVDPV type 1*
2004 2005 2006
3
9
2001
2002
2003
cVDPV type 2*
2004 2005 2006
3
22
2007
71
2008
66
2009
154
2010
27
1
6
13
5
2
15
1
1
5
1
18
1
2
2
3
2000
1
4
2001
2002
2011
13
12
4
5
1
3
2003
2004
Ethiopia
Cambodia
cVDPV type 3*
2005 2006
1
1
2007
2008
2009
1
2010
6
2011
Most recent
case
02-Jun-11
06-Dec-07
26-Oct-05
11-Nov-04
26-Jul-01
12-Jul-01
Most recent
case
28-Jun-11
09-Jun-11
24-Mar-11
20-Jan-11
10-Nov-10
13-Oct-10
01-Jun-10
18-Jan-10
16-Feb-09
13-Jul-05
Most recent
case
04-Nov-10
15-Jan-06
Vaccine-derived poliovirus (cVDPV) is associated with 2 or more cases of AFP. Niger 2006, Niger
2009, Niger 2010, Chad 2010 cVDPVs are
Paradosso
linked to the Nigeria outbreak. VDPV type 2 cases with greater than 5nt difference from sabin in VP1 and VDPV types 1 and 3 cases with greater than 9nt
Wild
difference from sabin in VP1 are reported here. Figures exclude VDPV from non-AFP source. Nigeria figures include the following cases with WPV1/cVPDV
2 mixture: 2005 – 2, 2006 - 1, 2007 - 1, 2008 – 3, 2009 - 1, 2011 – 1; WPV3/cVPDV2 mixture 2007 - 2.PV2 eradicato
1Circulating
*Figures include multiple emergences and transmission chains.
Data in WHO/HQ as of 30 Aug 2011
VDPVs in sewage
Data from Finland
Samples collected in Tampere
NB. IPV used exclusively in country except in 1984 to respond to WPV3 outbreak
Date of specimen
15-Dec-08
15-Jun-09
06-Jul-09
14-Sep-09
01-Feb-10
22-Mar-10
17-May-10
24-May-10
31-May-10
14-Jun-10
20-Sep-10
11-Oct-10
25-Oct-10
25-Jul-11
VDPV1
yes
yes
yes
yes
yes
yes
yes
yes
yes
Seotype of VDPV found
VDPV2
yes
yes
yes
yes
yes
yes
yes
yes
yes
yes
1 VDPV1 from Helwan, Cairo, Egypt sewage, 07 February 2010.
1 VDPV2 from Estonia, 25 November 2010
VDPV3
yes
yes
yes
yes
yes
yes
yes
yes
yes
VDPVs in sewage
Data from Israel
Multi-year detections of VDPV2
on 37 occasions during 12.5 years (between May 1998 and November 2010)
Site and cluster of detected VDPV2 (number of isolates)
Date
1
1A
1A1
1A3
Saf Dan
Reading
Kav B
Ayalon
1.6 million
0.8 million
1A3.2
1A3.3
1A3.4
1A3.5
1A3.6
1A4
1A5
Ayalon Yad
Eliahou
Ayalon
Rakevet
Ayalon
Hatkiva
Ayalon Park
Darom(103)
Ayalon Park
Darom(108)
Ayalon Park
Darom (109)
Ayalon (C-121)
0.05 million 0.35 million
3
Jerusalem
Haifa
0.75 million 0.27 million
15-Nov-10
1E7(1)
15-Nov-10
1E7(1)
24-Jun-10
1E6(1)
21-Apr-10
1E6(1)
27-Jan-10
1E5(2).1E6(2)
1E5(2),1E6(1)
20-Oct-09
1E4(3)
1E4(2)
30-Aug-09
2
1E4(1)
22-Feb-09
3(1)
20-Jan-09
1E3(1)
23-Dec-08
1E3(1)
25-Nov-08
2C(2)
17-Nov-08
1E3(1)
29-Jul-08
1E3(1)
1E4(1)
30-Jun-08
1E4(1)
1E4(1)
24-Jun-08
1E3(1)
24-Feb-08
1E2(5)
29-Jan-08
1E1(1), 1E2(1)
17-Sep-07
2C(1)
28-Aug-07
1E1(1)
27-Aug-07
1E1(1)
23-Jul-07
1E1(1)
20-Mar-07
1D(2)
06-Dec-06
2C(1)
18-Oct-06
1D(1)
04-Oct-06
2B(2)
06-Sep-06
1D(1)
09-Aug-06
1D(1)
14-Mar-06
2B(1)
2A(2)
02-Feb-06
2A (1)
20-Jul-05
1D(2)
13-Apr-05
1D(1)
22-Apr-04
1C(1)
15-Dec-99
1A(1)
06-Dec-99
1B(1)
03-Nov-99
1A(1)
06-Sep-99
1C(1)
05-May-98
1A(1)
1
2
3
4
NOTES:
37 samples positive for type 2. 1 for type 1
number of isolates in sample are in ().
The lineages were emerging. We have a better picture now
There are 4 genetic lineages for Group 1
TYPE 2 GROUP 1
TYPE 2 GROUP 2
TYPE 1 GROUP 3
Isolamento di (iVDPV) da soggetti con Immunodeficienza (1997-2009)
Casi = 42
Type 1
Type 2
Type 3
8 screening per casi iVDPV previsti nei Paesi in via di sviluppo
Added in 2009
• 1 Hypogamma case, Argentina with onset in 2009, alive, paralysed
• 1 CVID, USA, retrospectively detected, exposure ~ 13 years before, died
• 1 CVID, UK, onset 2000 retrospectively detected
Ricerca di
antivirali
NB. 3 cases mentioned at last meeting were not added: Tunisia (2), Russian Federation (1) based on follow-up findings
Reported iVDPVs, 2009 to April 2011
COUNTRY
ONSET
TYPE
COMMENT
Argentina
2009
VDPV 1
hypogammaglobulinemia
Colombia
10-Jul-09
VDPV 2
agammaglobulinemia
India
04-Sep-09
VDPV 1
hypogammaglobulinemia ?
India
29-Jan-10
VDPV 2
hypogammaglobulinemia ?
Iran
10-April-2007
VDPV 1
PID
Algeria
15-Apr-10
VDPV 2
hypogammaglobulinemia
Sri Lanka *
-
VDPV 2
SCID - non AFP
China
Feb-2011
VDPV 2
PID
China
Feb-2011
VDPV 3
PID
Egypt *
02- May-2011
VDPV 2
PID
VDPV 1
PID (sample collected 30-June2011). Deceased
VDPV 2
PID
Egypt *
Iran
14-May-2011
Iraq
2010
VDPV2
Immunodeficiency diagnosis on
clinical grounds, no testing done.
AFP
Turkey
2011
VDPV2
PID - Non-AFP patient
During > 50 years of OPV use, ~ 60 people with B–cell defects excreting iVDPV
Studies on iVDPV detection involving GPLN laboratories are ongoing
viruses shown with * from special studies
Soggetti con immunodeficienza “long-term excretors”
con isolamento di VDPVs
Country
Year
Age
(years)
UK
UK
Japan*
USA*
USA
UK
USA*
Germany*
UK
USA*
Argentina*
Germany*
Italy*
Taiwan*
Ireland
1962
1962
1977
1981
1986
1987
1990
1990
1995
1995
1998
2000
2000
2001
2002
3
20
3
17
11
34
1.3
7
25
5
3
24
1.75
8
1
Sex
Immune
deficiency
Polio
serotype
% VP1
drift
Last
OPV dose
Excreting
now?
m
f
m
m
f
m
?
m
m
f
m
f
f
m
m
hypogamma
hypogamma
XLA
cvid
cvid
cvid
scid
cvid
cvid
scid
agamma
ab deficiency
agamma
ab deficiency
?
1
3
2
1
2
2
2
1
2
2
1
1
2
1
1
?
2.3
?
10.0
10.8
4.1
1.8
8.3
12.1
2.2
2.0
3.5
0.9
3.4
1.5
32 months
21 months
2 years
7.5
9.6
>17 years
9 months
~8.5 years
>10 years
3.7 years
unvacc
2 years
1 year
2.5 years
9 months
no
no
no
no
?
yes
no
no
yes
no
no
yes
no
yes
yes
* Paralysis
Nucleotide variation in Sabin type 2 poliovirus from an immunodeficient patient with poliomyelitis.
Buttinelli G, Donati V, Fiore S, Marturano J, Plebani A, Balestri P, Soresina AR, Vivarelli R, Delpeyroux F, Martin J, Fiore L.
J Gen Virol. 2003;84:1215-21.
7079 IND 86
3825 PAK 91
Patient 1
Patient 2
2203 BAN 82
BeniSuef-93
9
EGY93-034
Giza-90-1
PER83-7834
4568-1 ISR
Giza-88
02-70003
04 078 342
04 212 161
04 292 173
Sabin 2
0864 GEO 87
16-3-95
16-1-98
16-6-95
29-3-95
21-10-95
0176 PER 89
11-1-02
26-3-04
SVK1432Z3
0317 EGY 55
0301 CAE 80
5890 VTN 88
0295 ISR 78
0297 EGP 79
2996 SWE 77
SVK1398Z1
Analisi filogenetica
isolati Polio tipo 2 da
Soggetti Immunodeficienti
Inghilterra
Ricerca
Lester M. Shulman, Danit Sofer, Yossi Manor, Ella Mendelson, Jean Balanant, Anna
Laura Salvati, Francis Delpeyroux, Lucia Fiore. Antiviral activity of 3(2H)- and 6chloro-3(2H)-Isoflavenes against highly diverged, neurovirulent vaccine-derived,
type 2 poliovirus environmental isolates (aVDPVs). PLoS One. 2011;6(5).
Nuove strategie per la vaccinazione “uso dell’IPV”
Standalone IPV
IPV - penta combo
IPV - hexa combo
Unknown
Not applicable
Data in WHO HQ as of Sep 2010
Paesi che usano il vaccino
Salk (IPV)
The boundaries and names shown and the designations used on this map do not imply the
expression of any opinion whatsoever on the part of the World Health Organization
concerning the legal status of any country, territory, city or area or of its authorities, or
concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent
approximate border lines for which there may not yet be full agreement.
WHO 2010. All rights reserved
Strategie per produrre vaccini Salk (IPV) meno costosi
Reduce number
of doses
Develop new
devices
Reduce antigen
content
Reduce
production cost
• Use fewer doses per schedule
• Develop intradermal (ID) device or microneedle patch to stretch doses
• Use adjuvant to reduce antigen contents per
dose
• Enables IPV production in developing countries
with less or non-infectious strain
Ritorno al passato
Riduzione dei finanziamenti 1988-2010: $7.13 billion
USAID
US CDC
France
G8
49%
Italy
Bangladesh
Germany
Indonesia
Russian
Federation
India
Pakistan
Japan
Multilateral
Sector
12%
European
Commission
Netherlands
IFFIm
Denmark
World Bank (India)
Sweden
Others
UN Foundation
Bill and Melinda Gates
Foundation
Non-G8
OECD/
Other 5%
Norway
WB Investment
Partnership for Polio
Private
Sector
20%
Domestic
Resources
14%
UK
Canada
Rotary
International
2009-10 Funding Gap:
US$ 345m of $1.34b budget
„Other‟: Governments of Angola, Austria, Australia, Belgium, Czech Republic, Finland, Hungary, Iceland, Ireland, Italy, Liechtenstein, Luxembourg, Malaysia,
Monaco, Namibia, New Zealand, Nigeria, Oman, Pakistan, Portugal, Qatar, Republic of Korea, Russian Federation, Saudi Arabia, Singapore, Spain,
Switzerland, Turkey, the United Arab Emirates; African Development Bank; AG Fund; American Red Cross; De Beers, Inter-American Development Bank,
Central Emergency Response Fund (CERF), International Federation of Red Cross and Red Crescent Societies, Oil for Food Programme, OPEC Fund,
Sanofi Pasteur; Saudi Arabian Red Crescent Society, Smith Kline Biologicals, UNICEF National Committees, UNICEF Regular and Other Resources, United
Arab Emirates Red Crescent Society, WHO Regular Budget and Wyeth.
Eradicazione globale della
poliomielite
Tappe
1988
Risoluzione WHA 41.28
2013 ?
Interruzione trasmissione
poliovirus selvaggi
2016 ?
Certificazione dell’eradicazione
globale della polio
2014-2016 ?
Interruzione della
vaccinazione con OPV
Ministero della Salute , Direzione Generale della Prevenzione, Ufficio Malattie Infettive
There is no question that the
eradication strategies work
when fully applied…
'We will complete
polio eradication!’
Margaret Chan
WHO Director General
…finishing eradication
depends fully on mobilizing
the political will to reach all
children.
Attività ISS/Ministero della Salute per il
mantenimento dello status polio-free dell’Italia
• Sorveglianza AFP
• Sorveglianza ambientale
• Sorveglianza soggetti immunodeficienti
• Contenimento dei poliovirus selvaggi e vaccino-derivati
SORVEGLIANZA ATTIVA DELLE PARALISI FLACCIDE ACUTE
IN ITALIA (1997-2012)
ISTITUTO SUPERIORE DI SANITA’
MINISTERO DELLA SALUTE
CRIVIB
Dir. Gen. Prevenzione Sanitaria
L. Fiore
F. Oleari
G. Buttinelli
S. Fiore
M.G. Pompa
E. Rizzuto
A. Battistone
Responsabili e Collaboratori dei
CENTRI DI REFERENZA REGIONALI
Referenti dei
PRESIDI OSPEDALIERI
Sorveglianza attiva delle paralisi flaccide acute in Italia
(1997-2006)
Sorveglianza attiva: ossia contatto diretto e continuativo tra
Referenti Regionali e centri ospedalieri.
Immediata notifica dei casi all'ISS e al Ministero della Salute.
Raccolta dei campioni clinici ed invio all'ISS per le analisi di
laboratorio.
Cinque Centri di referenza regionali effettuano le indagini
virologiche preliminari (Lombardia, Emilia-Romagna,
Liguria, Puglia e Sicilia)
Soggetti con agammaglobulinemia X recessiva in Italia
(vaccinati o non con OPV)
Pazienti arruolati:
(Età: 3 - 35 anni)
38
Medici segnalatori
Bologna
1
Dott.ssa Alvisi
Napoli
1
Prof. Pigneta
Bari
9
Dr. Martire/ Dr. Cardinale
Palermo
3
Dr. Trizzino
Catanzaro
1
Dr. Pozzi
Brescia
14
Prof. Plebani/ Prof.Ugazio*
Pavia
1
Dott.Bossi
Roma
4
Prof. Nigro
Firenze
4
Dott.ssa Azzari
Totale campioni feci prelevati: 66
Risultati tutti negativi all'isolamento per poliovirus ed altri enterovirus in colture
cellulari HEp-2C e RD
Buona copertura anticorpale verso i poliovirus (minore per il sierotipo1)
*Collaborazione con l’Associazione Italiana per le Immunodeficienze (AIEOP)
2003
L. Fiore et al. J. Clin. Imm. (2004), 111, 98-102
Pazienti arruolati: 18
Medici segnalatori
Pazienti arruolati: 14
Bari
Dr. B. Martire (Azienda Ospedaliera Policlinico di Bari)
Brescia 4
Palermo 2
4
Roma 14
Dott.ssa A.Pesce (Policlinico Umberto I - Roma)
Roma
Totale campioni feci prelevati : 21
Totale campioni di siero prelevati: 22
nei confronti dei 3 sierotipi di poliovirus
Dr. B. Martire (Azienda Ospedaliera Policlinico di Bari)
Dr. Trizzino (Dipartimento di Pediatria,
Ospedale G. di Cristina, Palermo)
Dott.ssa A.Pesce (Policlinico Umberto I - Roma)
Totale campioni feci prelevati: 16
Totale campioni di siero prelevati: 6
Campioni di feci: negativi all'isolamento per poliovirus
colture cellulari L20B e RD
uno positivo per Echovirus 18 (paziente Roma)
Campioni di siero: titoli anticorpali protettivi
8
Medici segnalatori
Campioni di feci: negativi all'isolamento per poliovirus
colture cellulari L20B e RD
2007
Campioni di siero: titoli anticorpali protettivi nei confronti
dei 3 sierotipi di poliovirus
2008
Progetto 2012 (ISS E OPBG)
Soggetti con agammaglobulinemia X recessiva in Italia
(vaccinati o non con OPV)
Coordinamento dei Medici Referenti
Ospedale Pediatrico Bambino Gesù
Dr.ssa Patrizia D’Argenio
Dr.ssa Maria Assunta Castelluzzo
Estendere la ricerca ad altri virus enterici quali i rotavirus, molto diffusi, e i
norovirus per i quali non é stata ancora valutata l'efficacia della terapia con
gammaglobuline
Convegno
SORVEGLIANZA DELLE PARALISI
FLACCIDE ACUTE IN ITALIA
3 dicembre
20042012
Roma
15-16 Marzo
BREVE STORIA DELLA VACCINAZIONE IN
ITALIA
• 1958 vaccino Salk su base volontaria
• 1964 vaccino Sabin su base volontaria
• 1966 vaccino Sabin obbligatorio
• 1999 schedula sequenziale IPV-OPV
• 2002 solo IPV (vaccino esavalente)
Poliomielite in Italia
1982
Ultimo caso notificato di poliomielite
da virus selvaggio in Campania
Poliomielite
in Italia
In un mondo globalizzato e
con i moderni mezzi di
trasporto tutti i paesi sono a
rischio di importazione di
virus polio selvaggi dai paesi
ancora endemici
Nigeria,Pakistan,Afghanistan
I bambini vaccinati con IPV sono
a rischio di re-infezione (scarsa
immunità mucosale) e potrebbero
trasmettere il virus a bambini non
vaccinati
In Italia non possiamo abbassare
la guardia!!
Occorre quindi vaccinare secondo
la schedula e senza ritardi e
intensificare le sorveglianze
Ringraziamenti
I Responsabili dei Centri di Riferimento Regionali e i loro collaboratori
Gli Assessorati alla Sanità Regionali
I Referenti Ospedalieri
I Referenti del Ministero della Salute
I Collaboratori del mio Reparto
La Segreteria del CRIVIB