TETRALOGIA DI FALLOT:
GENOTIPO E FENOTIPO
Gilda Caruso
Università di Bari
Incidenza e fenotipo “di base”
incidenza
¨
¨
¨
¨
3·5% dei neonati
con cardiopatia
congenita,
Non differenza di
sesso,
Causa sconosciuta,
Per lo più sporadica,
rischio di ricorrenza
del 3% se non ci
sono casi nei
familiari di 1°
grado.
Fenotipo “classico”
•Stenosi polmonare
•Div
•Destroposizione aortica
•Ipertrofia VD
Fenotipo classico ed età di
osservazione clinica
¨
Assenza di ipertrofia ventricolare
destra in età fetale
Oltre il fenotipo classico….
VARIANTI
¤
TOF con stenosi polmonare 76.7%
TOF con atresia polmonare 20.3%
¤
TOF con valvola polmonare assente 3%
¤
ANOMALIECARDIACHE ASSOCIATE
¤
¤
¤
¤
¤
Difetto interatriale
Arco aortico destro
Vena cava superiore sinistra
Canale Atrio-Ventricolare
IVA dalla coronaria destra
83%
25%
11%
8%
5%
TOF con atre s ia polmonare
t. di Fallot come “famiglia” di fenotipi
¨
¨
Simile anatomia
intracardiaca,
Ma alta variabilità in
termini di:
¤ Anatomia
dell’arteria
polmonare ecc.
¤ Anomalie associate
intra ed
extracardiache
¤ Esito clinico
Esiste anche una
famiglia di
genotipi?
ASSOCIAZIONI EXTRACARDIACHE e
ANOMALIE GENETICHE nel Fallot
Nelle serie pre-natali
Nelle serie post-natali:
¨
¨
20-25%
associati a cromosomopatie
n
¨
trisomia 13 e 21
40-45 %
associati a malformazioni
extracardiache
¨
il 20 % è associato
a cromosomopatie
¤ Trisomia 18 e 21,
¤ microdelezione 22q11
? 35%
associati a malformazioni
extracardiache
(più frequenti onfalocele, atresia
esofagea e duodenale, atresia anorettale)
¨
(Allan LD et al. JACC 1994) (Brown DLet al.
J Ultrasound Med 1993) (Ferencz. et al- 1993)
Microdelezione 22q11 e sindromi
¨
La delezione 22q11.2 è presente nella maggioranza di
casi di sindrome di:
DiGeorge
(DGS, 88%),
¤
Velocardiofaciale
(VCFS, 76%),
¤
Anomalia conotruncale e facciale
(CAFS, 80%)
¤
n
¤
¤
Aploinsufficienza del cr. 22 è riportata nelle sindromi di Opitz
e CHARGE
In tutte vi è simile incidenza di cardiopatie
congenite,
75–85% of patients with chromosome 22q11.2 microdeletion have congenital heart
disease, in particular ventricular septal defect, conotruncal abnormalities and aortic
arch abnormalities.
n
M. Earing et al. / Progress in Pediatric Cardiology 15 (2002) 119–123
¤
ma tipo e frequenza dei singoli difetti sono diversi
¤
Nella CAFS i più frequenti sono TOF (74%) e DIV(16%).
¤
Nella DGS i più frequenti sono interruzione dell’arco aortico
tipo B (41%) e TOF (29%).
microdelezione 22 q11,
t. di Fallot ed esito clinico
¨
Vi è un progressivo riconoscimento di substrati genetici del Fallot che possono
influenzare l’andamento post-chirurgico.
¤
¨
La microdelezione 22 q11 è presente sino al 25% dei casi, quindi va
sempre cercata nei soggetti con Fallot.
La microdelezione 22 q11 diventa sempre più importante non solo per le
manifestazioni cardiache e sindromiche, ma anche per l’associazione con malattie
psichiatriche ad esordio tardivo.
¤
Bassett e AL. hanno mostrato che adulti con la microdelezione 22q11
hanno un’incidenza di schizofrenia di circa il 25%, mentre circa l’1% dei
soggetti con schizofrenia hanno la delezione
n
Rauch R et al. Journal of medical genetics 2010 May
Correlazione genotipi-fenotipi nel
Fallot
¨
Studio genetico su 230 casi di Fallot.
n
n
¤
Ricerca delezione 22q11
Sequenziamento TBX1, NKX2.5 e JAG1.
Aberrazioni genetiche in 42 pazienti (18%),
n
La più frequente è la delezione 22q11.2 (7.4%), caratterizzata
da:
n
Ostruzione delle arterie polmonari prossimali
Ipoplasia delle arterie polmonari centrali
n
Anomalie della succlavia destra.
n
n
Seconda in ordine di frequenza dalla trisomia 21 (5.2%),
caratterizzata da:
n
n
Canale atrio-ventricolare completo, virtualmente assente nella delezione 22
Seguono altre mutazioni puntiformi (3%).
n
Rauch R et al. Journal of medical genetics 2010 May
Anomala origine
della succlavia
dx con decorso
retroesofageo
Pathogenesis of cono-truncal
anomalies
¨
Tissues forming the conotruncal region, the thymus and parathyroid glands have a common embryonic
origin at approximately the fourth week of gestation in the third and fourth pharyngeal pouches.
¨
The head, heart and thymus all have in common some contribution from the cephalic neural crest.
¨
In the heart, neural crest cells migrate into the outflow tract of the developing heart tube and form both
the aortopulmonary and conotruncal portions of the outflow septation complex.
¨
Recent data demonstrate that abnormal migration and interaction of the neural crest cells in these
regions are responsible for the associated anomalies observed with chromosome 22q11.2
microdeletion.
¨
Thus, abnormalities of the migration and interaction of the neural crest cells in these areas could cause
a variety of abnormalities of the aortic arch and the septation of the conotruncus.
The essential
of tetralogy
of Fallot
¨
RVOT:
¤
¤
location of the normal building blocks
abnormal location of the building blocks in the setting of tetralogy of
Fallot.
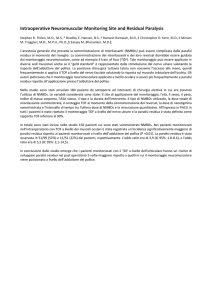
Comparison of RVOT
normal
tetralogy
CSV
VIF
TSM
AO
TSM
¨
¨
Infundibular septum (IS) inserts between the two
limbs (anterior and posterior) of the TSM
Fusion of the IS with the ventriculo-infundibolar
fold (VIF) to form the crista supraventricularis
(CSV)
¤
Outlet septum (OS) not recognizable (in yellow in
the cartoon)
¨
¨
¨
¨
Anterior and cephalad deviation of the outlet septum in
tetralogy
¤ Fusion with the anterior limb of the TSM
¤ Divorce between the VIF and CSV
Squeeze of the subpulmonary infundibulum between the
deviated OS and the septo-parietal trabeculations
Malalignment VSD
Overriding AO
Anatomical variations
¨
¨
¨
¨
¨
Degree of overriding of Ao
¤ From a-v concordance to
DORV
Morphology of the VSD
¤ 2/3 perimembranous
¤ 1/3 muscular
n Variable position of the
conducting system
Morphology of the subpulmonary infundibulum
¤ Variable hypoplasia and
lenght
Fibrous continuity between AoVTV-Membranous septum
Septo-parietal trabeculations
¤ Variable hypertrophy
¨
¨
¨
¨
Morphology of the pulmonary
valve
Peripheral stenosis of the
pulmonary arteries
RV hypertrophy
¤ Changes with age and with
the variant of ToF
Associated anomalies
¤ Right aortic arch
¤ Atrio-ventricular septal
defect
¤ MV anomalies
¤ others
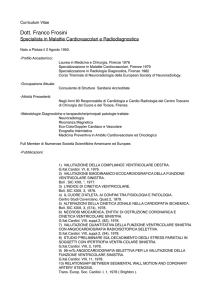
incuneamento dell’aorta tra
le valvole atrio-ventricolari
¨
¨
Wedge position of the
Ao valve in the normal
heart
Anteriorly positioned and
dextroposed Ao in
tetralogy
¨
Cuore normale
¨
Tetralogia di Fallot
Degree of overriding of Ao
a-v concordance
DORV
Morphology of the VSD
¨
¨
Between the branches of the TSM
More frequently perimembranous and subaortic
¨
¨
Fibrous continuity between Ao valve and TV valve
More rarely muscular and subaortic
Position of the conducting system
¨
¨
¨
Node on the postero-inferior border of the
perimembranous VSD
Penetrating bundle in the area of Ao-Tv continuity
(here Tv septal leaflet has been removed)
Branching bundle below the septal crest of the VSD
Haemorrhage in bundle branch
due to surgical trauma
Muscular VSD in ToF
¨
the muscular rim
¤ protects
the conduction axis
¤ is formed by fusion of the
postero-caudal limb of the
septomarginal trabeculation
with the ventriculo-infundibular
fold
¤ Ao-Tv are not in continuity
Rare variants
OS
¨
¨
Very rarely doubly committed and
subarterial VSD do to absent infundibular
septum
Ao-Pv continuity
¨
ToF associated with atrio-ventricular
septal defect
Subpulmonary obstruction
¨
produced in the setting of
deviation of the muscular
outlet septum,
¤ or
¨
¨
¨
its fibrous remnant,
coupled with an anomalous
arrangement of the
septoparietal
trabeculations,
combined with biventricular
origin of the aorta
and an interventricular
communication.
Subpulmonary obstruction
¨
¨
¨
Very short deviated outlet septum
Very narrow infundibulum
Hypertrophy of septoparietal bands
¨
¨
Extreme lenght of the
infundibular septum
Long and narrow outflow
Endocardial fibrosis
of pulmonary
infundibulum
Morphology of the pulmonary valve
¨
¨
¨
¨
Very often
bicuspid semilunar
valve
Rarely unicuspid
Rarely tricuspid
Often dysplastic
Absent pulmonary valve with ToF
morphology
Bronchial compression
Anomalies of the aortic arch
Left Ao arch
¨
Fetal pulmonary atresia with VSD
¤
Fallot’s morphology
Right Ao
arch
Pulmonary atresia with VSD
¨
¨
¨
Tetralogy-like morphology
Extreme form of the usual
ToF
Usually muscular type of
pulmonary atresia (absent
valve)
¤
OS
¨
¨
¨
Rare valvular atresia
Deviated outlet septum
Perimembranous VSD
Overriding Ao
Pulmonary blood supply
¨
Variations in morphology of
pulmonary blood supply
¤ Unifocal
supply via ductus
arteriosus
n
Confluent pulmonary arteries
¤ Multifocal
n
supply
Aorto-pulmonary collateral
arteries (MAPCs)
n
Generally without ductus
Unifocal supply
Atretic PT
Multifocal supply
MAPCAs from descending thoracic aorta
extending to the pulmonary hilum
Confluent PAs
Different compartments of the intrapulmonary
circulation fed by different sources
Ductus supplying both lungs
From 2 to 5 collaterals
Multifocal supply
¨
In the presence of MAPCAs
¤
¤
¤
¨
Atretic PT
Confluent PAs
The ductus may be present
Other sources:
¤
¤
¤
¤
Persistent fifth aortic arch
Ao-pulmonary window
Brachio-cephalic arteries
Coronary arteries
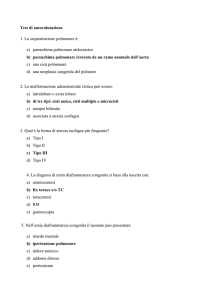
2° trimester fetal Pulmonary atresia with Tetralogy of
Fallot’s morphology with right aortic arch and MAPCA’s
MAPCA’s
rig ht ao rtic arc h