Novità in tema di
vaccinazione
antinfluenzale nell’adulto
Preparati al B!
Stefano Castagna
Medical Deparment Vaccines
GlaxoSmithKline Italia
Disclosures
•Stefano Castagna è dipendente
GlaxoSmithKline S.p.A.
Presentation title in footer
00 Month 0000
2
Presentation title in footer
00 Month 0000
3
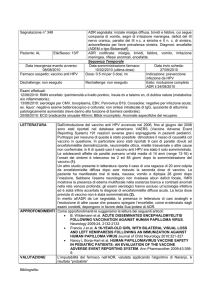
Vaccini Quadrivalenti attualmente in sviluppo
QIV1
Flumist® / Fluenz®2,3
Fluzone® /
Vaxigrip®4–6
QIV7
QIV8
Fluarix Tetra™ /
FluLaval Tetra™
Novartis
vaccines
AstraZeneca /
MedImmune
sanofi-aventis
Novavax
Medicago
GSK Vaccines
Phase
I/II
IV / III
III
II
II
IV
MOA
MF59-QIV
Q-LAIV
QIV
VLP-QIV
H5 VLP-QIV
QIV
Administration
IM injection
Nasal spray
IM injection
IM injection
IM injection
IM injection
Company
Efficacy
Effectiveness
Immunogenecity
B Immuno
Safety
Ages
investigated /
licensed
Contraindication
s and
restrictions
Lower Effect
High Effect
6–35 months
2–17 years /
18–49 years
6 months –
<9years /
9–17 years /
18–60 years
(≥65 years)
18–64 years
18–60 years
>35 months
Cant be used in
Immunosupressed,
Increased wheezing in
6-23M. Limited effect
in 18yr and above
Data available / being investigated
QIV, quadrivalent inactivated vaccine; Q-LAIV, quadrivalent live attenuated influenza vaccine; VLP, virus-like particle
1. Della Cioppa G, et al. Vaccine. 2011;29:8696–704; 2. Block SL, et al. Pediatr Infect Dis J. 2012;31:745–51; 3. Block SL, et al. Vaccine. 2011;29:9391–7; 4. sanofi-aventis. Available at
http://clinicaltrials.gov/ct2/show/NCT01218646 (accessed August 2012); 5. sanofi-aventis. Available at http://clinicaltrials.gov/ct2/show/NCT01240746 (accessed August 2012); 6. sanofi-aventis.
Available at http://clinicaltrials.gov/ct2/show/NCT01481454 (accessed August 2012); 7. Novavax. Available at http://clinicaltrials.gov/ct2/show/NCT01561768 (accessed August 2012); 8. Medicago.
Available at: http://clinicaltrials.gov/ct2/show/NCT01244867 (accessed August 2012).
Bisogni insoddisfatti dei vaccini influenzali
Da più di un decennio, la maggior parte delle patologie influenzali stagionali sono
state causate da quattro ceppi di influenza (due sottotipi A e due lineage B).1-4
Non esistono dati che descrivano un possibile effetto cross-protettivo tra i lineage
B come dimostrato invece tra tipi di A15
E’ difficile per le autorità sanitarie prevedere quale dei due lineage B includere nei
vaccini influenzali trivalenti (TIV), e nelle ultime dieci stagioni il lineage B
contenuto nei TIV è stato diverso da quello circolante (circa 50%).3,5,6
Quando il lineage contenuto nei TIV non ha concordanza con quello che
predomina nella circolazione questi vaccini sono meno efficaci e l’impatto della
patologia è maggiore.6–11
GSK’s QIVs è il primo vaccino antinfluenzale inattivato autorizzato per rispondere
al bisogno identificato di ridurre il B-lineage mismatch.12
1 US CDC. Types of Influenza Viruses. 2013. Available at: www.cdc.gov/flu/about/viruses/types.htm. Last accessed December 2013.
2 McCullers JA, Huber MC. Correlates of vaccine protection from influenza and its complications. Hum Vaccin Immunother. 2012;8:34–44.
3 Ambrose CS, Levin MJ. The rationale for quadrivalent influenza vaccines. Hum Vaccin Immunother. 2012;8:81-8.
4 Rota PA, Wallis TR, Harmon MW, et al. Cocirculation of two distinct evolutionary lineages of influenza type B virus since 1983. Virology. 1990;175(1):59-68.
5 Belshe RB. The need for quadrivalent vaccine against seasonal influenza. Vaccine. 2010;28(Suppl 4):D45–D53.
6 Reed C, Meltzer MI, Finelli L, et al. Public health impact of including two lineages of influenza B in a quadrivalent seasonal influenza vaccine. Vaccine. 2012;30:1993–98.
7 Belshe RB. Efficacy of live attenuated influenza vaccine in children against influenza B viruses by lineage and antigenic similarity. Vaccine. 2010;28:2149–56.
8 Heikkinen T, Heinonen S. et al. Effectiveness and safety of influenza vaccination in children: European perspective. Vaccine. 2011;29:7529-34.
9 Tricco A, et al . Comparing influenza vaccine efficacy against mismatched and matched strains: a systematic review and meta-analysis. BMC Med. 2013; 11: 153.
10 DiazGranados CA, Denis M, Plotkin S. Seasonal influenza vaccine efficacy and its determinants in children and non-elderly adults: a systematic review with meta-analyses of controlled trials. Vaccine. 2012;31:49-57.
11 Karve S, Meier G, Davis KL, et al. Influenza-related health care utilization and productivity losses during seasons with and without a match between the seasonal and vaccine virus B lineage. Vaccine. 2013;31:3370-88.
12 US FDA. December 14, 2012 Approval Letter- Fluarix Quadrivalent. 2012. Available at: http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm332484.htm
13 Lafond KE, Englund JA, Tam JS et al. Overview of Influenza Vaccines in Children. J Ped Infect Dis Soc 2013;x:1–11. DOI:10.1093/jpids/pit053 .
.
14 Neuzil KM, Zhu Y, Griffin MR, et al. Burden of interpandemic influenza in children younger than 5 years: a 25-year prospective study. J Infect Dis 2002; 185:147–52
15 Beran J, et al. Challenge of conducting a placebo-controlled randomized efficacy study for influenza vaccine in a season with low attack rate and a mismatched vaccine B strain: a concrete example. BMC Infect Dis 2009; 9: 2.
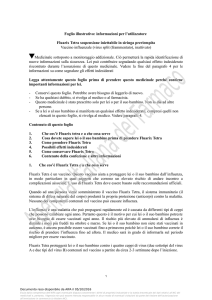
Storia della composizione dei
vaccini contro l’Influenza
2009 pandemico
1968 pandemico
“Swine” H1N1
1957 pandemico
H3N2
1918 pandemico
H2N2
Ri-emerge H1N1 stagionale
H1N1
H1N1
B-Victoria
Influenza B
B-Yamagata
Vaccini bivalenti (influenza A & B)
Vaccini Trivalenti
Vaccino quadrivalente
Vaccino monovalente influenza A
1920
1930
First isolation of
influenza A
virus
1940
1950
1960
1970
1980
1990
2000
2010
First isolation of
influenza B virus
6
McCullers JA, Huber VC. Hum Vaccin Immunother. 2012;8:34–44.
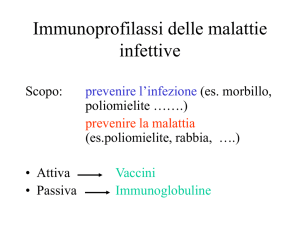
Epidemiologia EUROPA virus A e B
I 2 lineage B co-circolano dal 2000
100%
90%
80%
70%
60%
A/H1N1
A/H3N2
50%
B Yamagata
40%
B Victoria
30%
20%
10%
0%
2000-01
2002-03
2003-04
2004-05
2005-06
2006-07
2007-08
2008-09
2009-10
2010-11
2011-12
Adattato da European Centre for Disease Prevention and Control. Annual Epidemiological Report on Communicable Diseases in Europe.
Stockholm: ECDC. Anni 2000-2011
7
La patologia da Influenza B può essere seria
e solo parzialmente protetta dai TIV
• Maggior causa di epidemie ogni 2-4 anni 1,2
• Fino al 46% degli isolati influenzali dell’ultima decade sono stati di influenza B (range
<1-46%, avg. approx 23%)3
• Mortalità da Influenza B:
– 2° dopo A/H3N2, predominante nei soggetti >65 anni2
– Nel 2010-11, 38% (44/115) di tutti I decessi in età pediatrica associati all’influenza erano dovuti al tipo B4
• Le infezioni colpiscono tutte le fasce di età4–5
• La patologia è più comune negli bambini e adolescenti, ma le ospedalizzazioni e la
mortalità sono più comuni negli anziani4–5
In generale l’influenza B è una significativa causa di
assenteismo, visite cliniche, ospedalizzazioni e morte
1. Falcao IM, et al.. J Epidemiol Community Health 1998;52 (Suppl 1):39S–42S; 2. Thompson WW, et al. 2003;289:179–86; 3. Ambrose CS & Levin MJ. Hum
Vaccin Immunother. 2012;8:81–8; 4. Health Protection Agency. 2011. Available at http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1296687414154
(accessed September 2012).
5. Grant KA, et al. Commun Dis Intell. 2009;33:328–36; 6. Skowronski DM, et al. Vaccine. 2007;25:2842-51; 7. Gubbels S, et al. Epidemiol Infect. 2012 [Epub
ahead of print]; 8. Thompson WW, et al. Influenza Other Respi Viruses. 2009;3:37–49; 9. Finkelman BS, et al. PLoS One. 2007;2:e1296; 10. McBean AM &
Hebert PL. Int J Infect Dis 2004;8:227–35; 11. Zhou H, et al. Clin Infect Dis. 2012;54:1427–36
IBUS study (1997-2009):
Tassi mortalità attribuibili all’influenza per
tipo/sottotipo & stagione
Season
1997-1998
Flu A (H1)
0
Flu A (H3)
17350
Flu B
149
Total Influenza
17499
% Flu A
99%
% Flu B
1%
1998-1999
5
17479
6673
24158
72%
28%
1999-2000
11
21585
183
21780
99%
1%
2000-2001
205
342
11302
11849
5%
95%
2001-2002
12
22262
4697
26971
83%
17%
2002-2003
148
2495
9376
12019
22%
78%
2003-2004
0
28812
425
29237
99%
1%
2004-2005
0
17140
7030
24170
71%
29%
2005-2006
45
14531
4870
19445
75%
25%
2006-2007
292
5151
5609
11052
49%
51%
2007-2008
91
14749
11312
26152
57%
43%
2008-2009
125
641
4105
4872
16%
84%
Avg. season
78
13545
5478
19100
71%
29%
Matias G et al. Influenza Other Respir Viruses. 2014 Jun doi: 10.1111/irv.12258..
L’ influenza B è associata ad un sostanziale impatto della
patologia in tutte le classi di età (UK)
Assessment del burden dell’ influenza e altre infezioni respiratorie in UK1:
Maggior numero annuale di casi di influenza B nei bambini vs. anziani
Maggio numero annuale di decessi associati all’influenza B nella popolazione anziana
rispetto ai bambini
L’ Influenza B è associata con un sostanziale Burden in tutte le fascie di età
Visite MMG
Ospedalizzazioni
Decessi
236.000
194.000
2400
1400
84.000
1100
5
0
< 15 y
15 - 64 y
>65 y
Pitman et al. J Infect 2007;54:530–38.
< 15 y
15 - 64 y
>65 y
< 15 y
78
15 - 64 y
>65 y
Emerge il lineage Victoria
Mismatch in USA
Circulating influenza B lineage
Yamagata
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
*
YM
YM
YM
YM
VIC
Victoria
*
†
*
†
*
*
VIC
YM
YM
VIC
VIC
YM
VIC
VIC
VIC
*Vaccine mismatch (>60% mismatch); †Partial vaccine mismatch (<80% matched)
CDC MMWR 1999;48:374–8; CDC. MMWR 2000;49;375–81; Belshe RB. Vaccine 2010;28 (Suppl 4):D45–D53;
CDC. MMWR 2011;60;705–12; CDC. JAMA. 2012;308:8548.
Vaccine
lineage
Emerge il lineage Victoria
Mismatch in Europa
Circulating influenza B lineage
Yamagata
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Victoria
*
†
*
†
*
*
VIC
YM
YM
VIC
VIC
YM
†
VIC
VIC
VIC
Data not available
*Vaccine mismatch (>60% mismatch); †Partial vaccine mismatch (<80% matched)
Ambrose CS & Levin MJ. Hum Vaccin Immunother. 2012;8:81–8;
ECDC.. Available at http://www.ecdc.europa.eu/en/publications/Publications/120312-TER-Seasonal-influenza-risk-assessment.pdf (accessed September 2012).
Vaccine
lineage
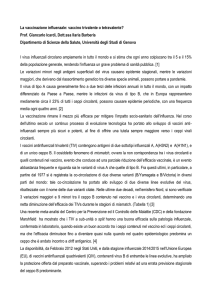
Composizione del vaccino per l’emisfero settentrionale e ceppi
circolanti di tipo B in Europa, in America ed in Liguria
In Liguria, un completo o parziale mismatching del tipo B, nell’ultima decade, si è
osservato, oltre che nella stagione 2001/021, negli inverni 2004/05, 2005/06,
2007/08 e 2008/09, quasi sempre riconducibile alla co-circolazione dei 2 lineage
1. Ansaldi F et al.
J Med Virol 2003;70:463-9
Efficacia dei vaccini antiinfluenzali trivalenti
Impatto del mismatch
Quando il ceppo B presente nei vaccini trivalenti non corrisponde al ceppo B
circolante e/o predominante, l'efficacia è relativamente bassa 2–5
1 Heikkinen T et al. Vaccine 29 (2011) 7529– 34. 2 Tricco AC et al. BMC Med 2013;11:153. 3 Dias Granados CA et al. Vaccine 2012;
31: 49– 57. 4 Belshe RB. Vaccine 2010; 28:2149–56. 5 Belshe RB. Vaccine 2010;28(Suppl 4):D45–D53.
New England Journal of Medicine 2013
Ogni anno, nel vaccino antiinfluenzale trivalente è
incorporato soltanto un singolo antigene del lineage
B che si prevede circolerà in quella stagione.
Questa scelta nella metà delle volte ha portato a
mismacth del B-lineage, rispetto al reale circolante.
Una potenziale soluzione per ridurre al minimo la
possibilità di una mancata corrispondenza del
B-lineage è quello di includere entrambi i B-lineage
nell’annuale vaccino contro l'influenza, come è
stato recentemente suggerito dal Advisory
Committee on Immunization Pratices del Centers
for Disease Controll and Prevention e dalla World
Health Organization.
16
Baden LR. For an influenza vaccine, are two Bs better than one? N Engl J Med 2013; DOI: 10.1056/NEJMe1315317
17
Allineamento globale per risolvere il
problema dell’influenza B
Febbraio 2013
Marzo 2012,
Febbraio 2012
Febbraio 2009
FDA discute la
possibilità
dell’inclusione di
un secondo ceppo
di influenza nei
vaccini
antinfluenzali1
2009
WHO raccomanda ai
produttori di considerare lo
sviluppo di vaccini
quadrivalenti con
l’inserimento del secondo
lineage B a partire dalla
stagione successiva
(2012/2013)2
2010
2011
EMA raccomanda
che 4 ceppi da
includere nella
vaccino della
stagione 2012/20133
2012
WHO emana chiare linee
guida per l’iserimento del
secondo ceppo B nel
vaccino della stagione
(2013/2014)4
2013
QIV, quadrivalent influenza vaccine; EMA, European Medicines Agency, EU; FDA: Food and Drug Administration, USA
1. FDA. http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/BloodVaccinesandOtherBiologics/VaccinesandRelatedBiologicalProductsAdvisoryCommittee/UCM167159.pdf (Accessed
August 2014); 2. WHO. www.who.int/influenza/vaccines/virus/recommendations/201202_recommendation.pdf (Accessed August 2014) ;
3. EMA. www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2012/03/news_detail_001467.jsp&mid=WC0b01ac058004d5c1 (Accessed August 2014);
4. WHO. http://www.who.int/influenza/vaccines/virus/recommendations/201302_recommendation.pdf?ua=1 (Accessed August 2014).
USA
“There are two antigenically distinct lineages of influenza B viruses, referred to as Victoria and
Yamagata lineages. Immunization against influenza B virus strains of one lineage
provides only limited cross-protection against strains in the other lineage. Given
this, and the challenge of predicting which B virus lineage will
predominate during a given season, inclusion of two B virus strains
(one from each lineage) in seasonal influenza vaccines may improve
protection against circulating seasonal B virus strains.”
“It is expected that the supply of IIV4 might be limited. Quadrivalent vaccines are designed
to provide broader protection against circulating influenza B viruses in
seasons during which the B virus contained in trivalent vaccines is
not an optimal match to the predominant circulating B viruses. However,
vaccination should not be delayed if only IIV3 is available. No preference is expressed for IIV4
over IIV3.”
IIV3 = trivalent inactivated influenza vaccine; IIV4 = quadrivalent inactivated influenza vaccine
US ACIP. Prevention and Control of Seasonal Influenza with Vaccines Recommendations of the Advisory Committee on Immunization Practices — United
States, 2013–2014. Morb Mortal Wkly Rep 2013; 62:1–43.
UK
“until most, if not all, influenza vaccine manufacturers are supplying quadrivalent
vaccines, it is unlikely that the number of doses of quadrivalent influenza vaccines
available would meet the total demand for influenza vaccines”
“Quadrivalent inactivated influenza vaccines are likely to provide better protection
against influenza B compared with trivalent inactivated influenza vaccines” 1
“Live attenuated influenza vaccine (LAIV) was more effective against infection than inactivated influenza
vaccines in children. Thus, LAIV should remain the vaccine of choice for children aged two to less than 18
years” 1
“The available quadrivalent inactivated vaccine should be the preferred vaccine
for those aged three years and older who cannot receive LAIV”1
Update June 2014 JCVI minutes (not yet in Green Book):
“After consideration of the data the Committee concluded that, all other factors being
equal, QIV was preferable to trivalent inactivated influenza vaccine (TIV). However
conclusions could not be drawn on the cost-effectiveness of QIV over TIV, from data
provided by the sole manufacturer of QIV.” 2
QIV = quadrivalent inactivated influenza vaccine
1. UK JCVI. Draft Minutes of June 2013 Meeting. Available at: https://www.gov.uk/government/policy-advisory-groups/joint-committee-on-vaccination-andimmunisation (Accessed August 2014); 2. UK JVCI Minutes of June 2014 meeting https://www.gov.uk/government/groups/joint-committee-on-vaccination-andimmunisation#minutes (Accessed August 2014).
Sommario delle raccomandazioni QIV
Paese/
Istituzione
Tipo di
raccomandazione
Gruppo(i) raccomandati
Global / WHO1
Permissiva*
Pregnant women, health care workers, children <5 years, elderly >65
years, chronic conditions
USA / ACIP2
Permissiva
Children (6 Mo+) & Adults
Canada / NACI3
Permissiva
Children (6 Mo+) & Adults
Preferenziale†
a. Elderly ≥65 years; Chronic conditions risk groups, Pregnant
women
b. Children (3-17 years)
Germany / DTG
Reiseimpfungen5
Preferentzale
Travelers >60 years, with co-morbid conditions, compromised immune
system
Germany / STIKO6
Pre-permissiva
Pregnant women, health care workers, children <5 years, elderly >65
years, chronic conditions
France / Haut Conseil de la
santé publique 7
Permissiva
Children (≥3 years) & Adults
Hong Kong / Center for
Health Protection8
Permissiva
Children (≥3 years) & Adults
Taiwan / CDC Taiwan9
Preferenziale
Health care workers, Elderly >65 years, School children (6-18 years)
UK /
JCVI4
*Permissive recommendation = QIV may be used in place of TIV where available, but no preference expressed
†Preferential recommendation = Firm preference expressed for use of QIV over TIV, where available
See slide notes for references
Circolare Min sal 2014-2015
http://www.trovanorme.salute.gov.it/renderNormsanPdf.spring;jsessionid=a9mgTGhOvAMBL2xH4l57jg**?codLeg=39451&parte=1&serie=&a
nno=0
Materiale di training ad esclusivo uso interno
Circolare Min sal 2014-2015
http://www.trovanorme.salute.gov.it/renderNormsanPdf.spring;jsessionid=a9mgTGhOvAMBL2xH4l57jg**?codLeg=39451&parte=1&serie=&a
nno=0
Materiale di training ad esclusivo uso interno
Circolare Min sal 2014-2015
http://www.trovanorme.salute.gov.it/renderNormsanPdf.spring;jsessionid=a9mgTGhOvAMBL2xH4l57jg**?codLeg=39451&parte=1&serie=&a
nno=0
Materiale di training ad esclusivo uso interno
Punti chiave nel predisporre un modello per valutare l'impatto e i
benefici di QIV
Quale è l’addizionale beneficio in termini di salute del QIV vs. vaccini
trivalenti (TIV) ciascun anno a livello di popolazione, in termini di:
Casi evitati
Ospedalizzazioni evitate
Decessi evitati
Benefici del
QIV per
Salute
Pubblica
Impatto del vaccino nel bloccare la catena di trasmissione
Herd effect: interazioni tra diversi gruppi di età
Quali sono i costi addizionali correlati all’influenza evitati con QIV
versus TIV:
Costi relativi ai casi di influenza , visite mediche, ricoveri e giornate
lavorative perse
E’ costo efficace implementare ogni anno la vaccinazione con QIV al
posto di TIV?
Quali sono I costi incrementali di QIV versus TIV ogni anno?
Qual’è il Rapporto incrementale di costo efficacia (ICER) del QIV vs. TIV?
Quale è l’impatto sul budget sanitario dell’introduzione del QIV?
Impatto
economico
di QIV
comparato ai
benefici
Un occhio al passato
Se QIV fosse stato disponibile
nell‘ultima decade…
Stima dell’impatto addizionale di QIV negli ultimi 10
anni
• Impact on influenza related health outcomes:
Rates of illness, hospitalization, and death Impact over 10
previous influenza seasons (1999/2000–2008/2009)
Risultati In USA, QIV could avrebbe ridotto ogni anno (media):
● 340,000 Casi (range: 2,242 - 1,325,828)
● 2,700 Ospedalizatzoni (range: 14 - 12,472)
● 170 Decessi (range: 1–663)
Reed C. et al. Vaccine 2012; 30:1993–1998
Impatto potenziale della vaccinazione dei gruppi a rischio e >65
anni con QIV negli ultimi 10 anni in UK
‘Modello Costo-utilità’, ipotizzando outcome in tutta la
popolazione UK (62,261,967)
Media stagioni degli
ultimi 10 anni
2005/06
(99% mismatch tra vaccino
e lineage B circolante)
COST (£)
Riduzione dei casi di influenza
17,088
COST (£)
100,296
Riduzione visite mediche
5121
198,484
30,056
1,164,971
Riduzione ospedalizzazioni
337
630,151
1,976
3,698,568
Vite salvate (Riduzione decessi)
168
Van Bellinghen LA, et al. PLoS ONE 2014 ; 9:e98437. doi:10.1371/journal.pone.0098437
988
Un occhio al futuro
Quando QIV sarà disponibile, che cosa
comporterà…?
Impatto economico del
vaccino antinfluenzale
quadrivalente
comparato al vaccino
trivalente: analisi di
costo-efficacia e di
impatto sul budget
M. Barbieri*, S. Boccalini, R.
Silvestri, F. Kheiraoui, C. de Waure,
P. Bonanni
* Centre for Health Economics,
York, UK
Tutto questo si trasforma in un reale vantaggio economico?
QUADRIVALENT VERSUS TRIVALENT INFLUENZA VACCINE: IS IT GOOD VALUE FOR MONEY?
Barbieri M1;Patarnello F2;Boccalini S3;Silvestri R2;Lapinet JA2;Tosatto R2;Kheiraoui F4;de Waure C4;Bonanni P3, Ricciardi WG4
ISPOR 2013
Programma di sviluppo clinico QIV Phase III
Q-QIV and D-QIV: Due sviluppi paralleli
Q-QIV
Q-QIV 003: Pediatric NI in 3–17 years and
immuno/safety in 6–35 m (N=3,000)
Q-QIV 007: Adult NI study
≥18y (N=1,600)
Q-QIV 006: Pediatric efficacy
study in 3–8 years (N=5,200)
QIV
clinical
development
plan
2010
2011
Arrows indicate study start
Q-QIV 012 Pediatric NI vs
D-QIV in 6-35m (~2,000)
2013--14--15--16
D-QIV licensed for age 3 year +
D-QIV 008: Adult NI study
in ≥18 years (N=4,600)
D-QIV
2012
Q-QIV 013: Immuno, safety
vs Fluarix in 6-35m (N=600)
D-QIV 004: Pediatric efficacy study
in 6–35 months (N=8,200)
D-QIV 003: Pediatric NI in 3–17 years and
immuno/safety in 6–35 m (N=3,000)
Conclusioni
• L’influenza B è una patologia severe e potenzialmente fatale in tutte le fasce di età
• E’ difficile prevedere quale sarà il ceppo circolante nella stagione successiva e in
ogni caso si crea un certo grado di mismatch B tra i virus contenuto nel TIV e quello
circolante nella popolazione
– Negli ultimi 10 anni in europa si è avuto un mismatch totale o parziale in oltre il 50% delle
stagioni
• La protezione verso l’influenza B è ottimale quando c’è concordanza tra il ceppo
contenuto nel TIV e quello circolante
• Lo sviluppo di un nuovo vaccino antinfluenzale quadrivalente, come raccomandato
(WHO, ECDC ecc.) rappresenta una risposta innovativa nel percorso di miglioramento
dell’efficacia dei vaccini antinfluenzali
• Il vaccino QIV ha dimostrato una risposta immune superiore per il ceppo B
addizionale rispetto al TIV, senza interferire con la risposta immunitaria degli altri 3
ceppi (A e B) contenuti nel vaccino, e senza alterare il profilo di sicurezza
• La vaccinazione con il QIV vs TIV ha dimostrato di Ridurre i casi di influenza ed il
relativo burden della patologia con un favorevole impatto economico che è risultato
essere costo efficace (inferiore al valore soglia di 50000 €/QALY)
41
Grazie per l’attenzione!
Let’s decide the 2014-2015 influenza vaccine composition!
GSK D-QIV Clinical Development Plan
Key studies objectives – Design – results – summary
GSK’s Quadrivalent Influenza Vaccine Development
Vaccines manufactured in Quebec and Dresden
Q-QIV
n:13100
Q-QIV 003: Non-inferiority/ safety in 3–17 years
and immuno + safety in 6–35 months (N=3,000)
Q-QIV 022 Non-inferiority vs
Fluzone in 6–35 months
(n=2400)
(Quebec)
Completed
Q-QIV 007: Noninferiority/safety/consistency in adults
≥18years (N=1,600)
Q-QIV 013: Immuno/ safety vs Fluarix
in 6–35 months (N=600)
Ongoing
Planned
2008
2009
2010
2011
D-QIV
n: 24100
(Dresden)
2012
2013
D-QIV 004: Efficacy in children
6–35 months (N=12,000).
Results 2015
D-QIV 002
Primed/unprimed
18-47 mo (N=584)
D-QIV 001
FTIH in adults
≥18 years
(PhII, N=420)
Q-QIV 021 Non-inferiority vs
Fluzone in 6–35 months
(n=300). Under analysis
Q-QIV 006: Efficacy
in children 3–8 years
(N=5,200)
D-QIV 008: Non-inferiority/
safety/consistency in adults
≥18 years (N=4,600)
D-QIV 003: Non-inferiority/ safety in
3–17 years and immuno/safety in 6–
35 m (N=3,000)
D-QIV 009:
D-QIV-004 booster
(n:400)
ZOS 004: Coadmin >50 years
(N=828) (+1 y follow up for
safety)
2014
D-QIV 015 (6m-49y)
(n: 2000) Yield Imprvt
D-QIV 010: Pneumovax
co-ad Immuno/ safety,
adults >50 years (n:350)
Confidential
GSK’s Quadrivalent Influenza Vaccine: D-QIV
GSK’s quadrivalent influenza vaccine: Fluarix® Tetra is manufactured in Dresden, Germany (DQIV) and is based on the trivalent formulation (Fluarix®), also manufactured in Dresden (D-TIV)
Indications/Licence:
D-TIV is licensed in the EU from 6 months of age
D-QIV is licensed from 3 years of age
1. Kieninger D et al. BMC Infect Dis 2013; 13:343; 2. EMC. 2013 Fluarix® suspension for injection in a pre-filled syringe. Package leaflet; 3. EMC. 2013 Fluarix®
Tetra suspension for injection in a pre-filled syringe.
GSK D-QIV: composition
QIV Vaccine
4
3
2
1
A-H1N1
B-Victoria
A-H3N2
B-Yamagata
One 0.5 mL dose of the split inactivated vaccine contains
15 μg haemagglutinin (HA) for each of the four influenza
virus strains, for a total of 60 μg HA
US FDA. 2013 Fluarix Quadrivalent Highlights of Prescribing Information.
Key pivotal trials:
Two pivotal phase III studies - Objectives
Children: D-QIV-0031
Adults: D-QIV-0082
• Confirm immunogenic superiority of
QIV for the added B strain vs. two TIV
formulations in 3–17 year olds
• Confirm immunogenic superiority
of QIV for the added B strain vs. two TIV
formulations in ≥18 year olds
• Confirm immunogenic non-inferiority of
QIV for the three common strains
shared with each of the two TIVs
• Confirm immunogenic non-inferiority of
QIV for the three common strains
shared with each of the two TIVs
• Describe reactogenicity and safety
Describe reactogenicity and safety
• Descriptive immunogenicity parameters Descriptive immunogenicity parameters
Demonstrate QIV production lot
consistency
1. Domachowske J et al. J Infect Dis 2013; 207:1878–87; 2. Kieninger D et al. BMC Infect Dis 2013; 13:343.
Key pivotal trials:
Two pivotal phase III studies - Designs
Children: D-QIV-0031
Adults: D-QIV-0082
• Randomised, controlled trial in
3–17 year olds; age stratified 3–8 years,
9–17 years
• Randomised, controlled trial in individuals
aged 18 years or over;
age stratified 18–64 years, ≥64 years
• N=3015
• N=4656
• Three groups: QIV, TIV-Vic and
TIV-Yam
• Three groups: QIV, TIV-Vic and
TIV-Yam
• Conducted in five countries in 2010–2011
• Conducted in six countries in 2010–2011
• Primed subjects received one dose and
unprimed subjects two doses
• Each subject received one dose
• Blood samples collected pre- and postvaccination
• Blood samples collected pre- and postvaccination
• Reactogenicity and safety (days 7 and 28,
and at 6 months)
• Reactogenicity and safety (days 7 and
21, and at 6 months)
1. Domachowske J et al. J Infect Dis 2013; 207:1878–87; 2. Kieninger D et al. BMC Infect Dis 2013; 13:343.
Key pivotal trials:
Study vaccine groups in paediatric & adult studies
A-type
B-type
Vaccine
groups
A-subtype
A-subtype
B-lineage
(Victoria)
B-lineage
(Yamagata)
D-QIV
A-H1N1
A-H3N2
B-Victoria
B-Yamagata
TIV (VIC)
A-H1N1
A-H3N2
B-Victoria
--
TIV (YAM)
A-H1N1
A-H3N2
--
B-Yamagata
1. Domachowske J et al. J Infect Dis 2013; 207:1878–87; 2. Kieninger D et al. BMC Infect Dis 2013; 13:343.
Study results in children: (3–17 years of age)
Haemagglutination-inhibition (HI) antibody response
D-QIV
TIV (Vic)
TIV (Yam)
Geometric mean titre (95% CI)
700
600
500
400
300
200
100
0
PRE
POST
H1N1
PRE
POST
H3N2
PRE
POST
B-Victoria
Per protocol immunogenicity cohort: D-QIV n=791, TIV-Vic n=819, TIV-Yam n=801
Geometric mean titres at Day 0 (PRE) and Day 28 (POST)
Domachowske J et al. J Infect Dis 2013; 207:1878–87.
PRE
POST
B-Yamagata
Study results in adults: (≥18 years)
Haemagglutination-inhibition (HI) antibody response
Geometric mean titres (95% CI)
D-QIV
TIV (Vic)
TIV (Yam)
700
600
500
400
300
200
100
0
PRE
POST
PI(D21)
H1N1
PRE
PI(D21)
POST
H3N2
PRE
POST
PI(D21)
PRE
B-Victoria
Per protocol
protocol immunogenicity
immunogenicity cohort:
cohort: D-QIV
D-QIV n=1809,
n=1809, TIV-Vic
TIV-Vic n=608,
n=608, TIV-Yam
TIV-Yam n=534
n=534
Per
Day 0 (PRE)
andtitres
Day 21
(POST).
Geometric
mean
at Day
0 (PRE) and Day 21 (POST).
Kieninger D et al. BMC Infect Dis 2013; 13:343.
PI(D21)
POST
B-Yamagata
Results in children and adults
Superiority: immune response
Immune response of D-QIV compared with trivalent influenza vaccines for the
added B strains
0000
Children 1
Adults2
GMT ratios
B-Yamagata antibodies: D-QIV vs. TIV-Vic
2.5 x
1.6 x
B-Victoria antibodies: D-QIV vs. TIV-Yam
2.8 x
1.6 x
B-Yamagata antibodies: D-QIV vs. TIV-Vic
35.5%
16.1%
B-Victoria antibodies: D-QIV vs. TIV-Yam
40.4%
10.5%
Difference in seroconversion rates*
*Seroconversion rate is defined as the percentage with either a pre-vaccination titre <1:10 and a postvaccination titre ≥1:40 or a pre-vaccination titre ≥1:10 and at least a four-fold increase in post-vaccination titre
1. Domachowske J et al. J Infect Dis 2013; 207:1878–87; 2. GSK Data on File 2013, Clinical Study Report 113275 (FLU D-QIV-003); 3. Kieninger D et al. BMC
Infect Dis 2013; 13:343; 4. GSK Data on File 2013, Clinical Study Report 114269 (FLU D-QIV-008).
Safety: reactogenicity in children (3–17 years)
Symptoms (Any, General, Local)
D-QIV
TIV (Vic)
TIV (Yam)
100
Symptoms post-dose 1
(% of subjects)
80
During 7 days postvaccination
60
40
20
0
All
Grade 3
Any symptoms
All
Grade 3
General symptoms
All
Grade 3
Local symptoms
1. Domachowske J et al. J Infect Dis 2013; 207:1878–87; 2. GSK Data on File 2013, Clinical Study Report 113275 (FLU D-QIV-003).
Safety: reactogenicity in adults (≥18 years)
Symptoms (Any, General, Local)
D-QIV
100
TIV (Vic)
TIV (Yam)
90
Symptoms
(% subjects)
80
During 7 days postvaccination
70
60
50
40
30
20
10
0
All
Grade 3
Any symptoms
All
Grade 3
General symptoms
All
Grade 3
Local symptoms
1. Kieninger D et al. BMC Infect Dis 2013; 13:343; 2. GSK Data on File 2013, Clinical Study Report 114269 (FLU D-QIV-008).
Fluarix™ Tetra (D-QIV) pivotal phase III Key
Studies Objectives - Summary
Paediatric 3–17 years
n=3015: Study D-QIV-003
•
•
•
•
Age stratified 3–8 years, n=1791
And 9–17 years , n=946
Primed subjects: 1 dose
Un-primed: two doses
Three groups: QIV, TIV-Vic and TIV-Yam
Adult and older adults ≥18
years, n=4656: study D-QIV-008
Endpoint
• Age stratified 18–64 years, n=2326
• And ≥65 years , n=2330
• One vaccine dose
Three groups: QIV, TIV-Vic and TIV-Yam
Confirm immunogenic superiority of QIV for the added B strain
vs. TIVs
Met
Confirm immunogenic non-inferiority of QIV for the three
common strains shared with each of the two TIVs
Met
Describe reactogenicity and safety
~TIV
Demonstrate consistency of
production of QIV lots
Met
1. Domachowske J et al. J Infect Dis 2013; 207:1878–87; 2. Kieninger D et al. BMC Infect Dis 2013; 13:343; 3. Safety and Immunogenicity Study of GSK Biologicals' Seasonal
Influenza Candidate Vaccine (GSK2321138A) Available at: http://clinicaltrial.gov/ct2/show/NCT01204671; (Accessed September 2014); 4. Immunogenicity and Safety Study of
GSK Biologicals' Influenza Vaccine When Administered in Children Available at: http://clinicaltrial.gov/ct2/show/NCT01196988 (Accessed September 2014).
Current status of global approvals and
licenses for GSK QIV manufactured in
Dresden
2012
US FDA
2013
USA
EMA
2014
Taiwan
Czech
Republic
UK
Spain
Macau
Luxembourg
WHO
Hong Kong
EMAP
Italy
LATAM
TECHNICAL
RECOMMENDATIONS
SUPPORTING QIV1-3
Germany
Belgium
France
Switzerland
Australia
Turkey
Israel
Approved/licensed4-20
Approval/license pending or submission in preparation
See slide notes for references
Conclusion
D-QIV : Fluarix™ Tetra is the 1st seasonal inactivated quadrivalent
influenza vaccine to be licensed
Immunogenicity has been studied in more than 24 000 subjects, where
more than 12 000 subject have been exposed to D-QIV
Clinical trials and data generated vs TIV in adults and children showed
that Fluarix™ Tetra immunogenicity is:
Non-inferior to Fluarix™ trivalent vaccine for shared strains
Superior for the additional B strain present in Fluarix™ Tetra
Acceptable safety profile similar to that of TIV
Studies are still on-going: efficacy study in children younger than 3
1. Kieninger D et al. BMC Infect Dis 2013; 13:343; 2. Domachowske J et al. J Infect Dis 2013; 207:1878–87 EMC. 2013 Fluarix® suspension for injection in a
pre-filled syringe. Package leaflet; 3. EMC 2013 Fluarix® Tetra suspension for injection in a pre-filled syringe. Package leaflet. Fluarix™ and Fluarix™ Tetra are
trademarks of the GlaxoSmithKline group of companies.; ; 4. ClinicalTrials.gov. An Efficacy Study of GlaxoSmithKline (GSK) Biologicals' Candidate Influenza
Vaccine GSK2321138A in Children. Available at: http://clinicaltrial.gov/ct2/show/NCT01439360. (Accessed September 2014).
Why do we need health economic
models?
Objective:
Health economic models aim at simulating the clinical and economic impact of an
immunization program
Is the intervention worth the money?
What is the most appropriate alternative?
For QIV they are required since:
Limited real-life data (i.e. effectiveness data)
Epidemiological data of influenza B not available for all countries/ regions
Limited number of QIV clinical trials/ immunogenicity
To explore QIV’s impact on indirect protection (‘herd protection’)
Cost of influenza and
its complications
Epidemiology
(attack rate, excess
hospitalizations and deaths)
Demographics
(pop. size, life expectancy,
utility, % of at-risk people)
Jit M, et al. Hum Vaccin Immunother. 2013; 4: 834-40.
Vaccines coverage rates
and vaccine price
Health
economics
model
Vaccine effectiveness
What is an economic evaluation?
Comparative assessment of both costs and consequences of two or several health care
interventions
Outputs:
Economic
Outputs:
Health benefit
Vaccination
Total cost avoided:
Direct cost+
Indirect cost
Cost of vaccination
e.g.
LYG
QALYs
QoL
Perfect QoL
QALYs gained
ICER =
Costintervention – Costcomparator
Effectintervention – Effectcomparator
Quality
of life
Death=
0
Today
Without
intervention
Remaining life
expectancy
With
intervention
Time
QALY, quality adjusted life year; LYG, life year gained; ICER, incremental cost-effectiveness ratio
Briggs A, Claxton K, Sculpher M. Decision Modelling for Health Economic Evaluation. Oxford, United Kingdom: Oxford University Press; 2007.(page 122 & 123)
The cost-effectiveness plane:
Results interpretation
Acceptability is relative
Cost ↑
Effect ↓
Incremental costs
Dominance to reject
0
Cost ↑
Effect ↑
COSTEFFECTIVE
Decision depends on financer’s willingness to pay : $50,000, $100,000,
€50,000, £30,000, or three times the per capita GDP of the country
Strategy of interest may be cost-effective
Incremental effects
Cost ↓
Effect ↓
Decision depends on financer’s
willingness to pay
Acceptability is relative
Cost ↓
Effect ↑
COST-SAVING
Dominance to accept
Briggs A, Claxton K, Sculpher M. Decision Modelling for Health Economic Evaluation. Oxford, United Kingdom: Oxford University Press; 2007.(page 122 & 123)
Key questions tackled by modeling
the impact and benefits of QIV
What is the additional health benefit of QIV vs. trivalent
influenza vaccine (TIV) each year at the population level, in
terms of:
Cases avoided
Hospitalizations avoided
Public health
benefits of
QIV
Deaths avoided
Vaccine impact on blocking the chain of transmission
Herd effect: Interaction between age groups
What are the additional influenza related costs avoided with
QIV versus TIV:
Cost of influenza cases, GP visits, hospitalizations, productivity
losses avoided
Is it cost-effective to fund QIV every year instead of TIV?
What is the incremental cost of QIV versus TIV over 1 year?
Economic
impact of
QIV
compared to
its benefits
Overall conclusions
Two influenza B lineages have been co-circulating in the last decade
A substantial mismatch has occurred between the influenza B virus represented in the seasonal
vaccine and the circulating strain
Fluarix Tetra® (D-QIV) has shown superior immunogenicity compared with TIV for the additional B
strain with a similar safety profile to TIV
Fluarix Tetra® (D-QIV) offers broader coverage than TIV, and has also been estimated to be costeffective compared to TIV in a UK model
For UK only
Prescribing Information – Refer to SmPC before prescribing.
Fluarix Tetra ▼Influenza vaccine (inactivated, split virion). Indication:
prophylaxis of influenza. Dosage and administration: Adults and children aged
≥36 months, previously vaccinated: 0.5 ml for i.m injection. Children aged
36months to <9years: not previously vaccinated, require a second 0.5ml dose at
least 4 weeks after. Children <3years: safety and efficacy has not been
established. Side effects: See SmPC for full details. Very common: irritability,
myalgia, injection site pain, fatigue, Common: appetite loss, drowsiness,
headache, gastrointestinal symptoms, arthralgia, injection site redness,
induration and swelling, shivering, fever, sweating. Serious: Guillain Barré
syndrome, acute disseminated encephalomyelitis, anaphylaxis and angioedema.
Precautions and contraindications: hypersensitivity to components including
eggs. Postpone in case of febrile illness. Pregnancy: can be used in all stages
of pregnancy and during breastfeeding. Legal category: POM Presentation
and Basic NHS cost: Fluarix Tetra 0.5 ml pre-filled syringe. 10 = £99.40,
1=£9.94 MA No. PL 10592/0302. MAH: SmithKline Beecham Limited trading as
GlaxoSmithKline UK, Stockley Park West, Uxbridge, Middlesex, UB11 1BT.
Further information is available from: Customer Contact Centre,
GlaxoSmithKline, Stockley Park West, Uxbridge, Middlesex, UB11 1BT;
[email protected]; Freephone: 0800 221 441. Fluarix is a trademark
of the GlaxoSmithKline group of companies. Date of preparation: May 2014.
UK/FLU6/0021/14
Adverse events should be reported. For the UK, reporting forms and
information can be found at www.mhra.gov.uk/yellowcard. For Ireland,
adverse events should be reported directly to the IMB; Pharmacovigilance
Section, Irish Medicines Board, Kevin O'Malley House, Earlsfort Centre,
Earlsfort Terrace, Dublin 2, Tel: +353 1 6764971. Adverse events should
also be reported to GlaxoSmithKline on 0800 221 441 in the UK or 1800 244
255 in Ireland
For Belgium, Czech Republic, France, Germany, Italy, Israel, Luxembourg, Spain, Switzerland,
Turkey, and USA:
ABBREVIATED PRESCRIBING INFORMATION: (Refer to the full Summary of Product Characteristics
before prescribing)
Name of medicinal product: Fluarix Tetra (Czech Republic, France, Italy, Luxembourg, Spain
Switzwerland, Turkey); Alpharix Tetra (Belgium); Influsplit Tetra (Germany); Fluarix Quadrivalent (USA)
Description: Suspension for injection in pre-filled syringe Influenza vaccine (split virion, inactivated).
Qualitative and quantitative composition: Each 0.5 ml dose contains Influenza virus (inactivated, split)
of the following strains*: A/California/7/2009 (H1N1)pdm09-like strain used (NIB-74xp) derived from
A/Christchurch/16/2010 15 micrograms HA**, A/Texas/50/2012 (H3N2) derived strains used (NYMC X223A) 15 micrograms HA**, B/Massachusetts/02/2012 derived strain used (NYMC BX-51B) (Yamagata
lineage) 15 micrograms HA**, B/Brisbane/60/2008 (Victoria lineage) 15 micrograms HA**.
This vaccine complies with the WHO recommendation (northern hemisphere) and EU decision for the
2014/2015 season. Fluarix Tetra may contain traces of eggs (such as ovalbumin, chicken proteins),
formaldehyde, gentamicin sulphate and sodium deoxycholate which are used during the manufacturing
process. *propagated in fertilized hens’ eggs from healthy chicken flocks. **haemagglutinin. Uses: Fluarix
Tetra is indicated for active immunisation of adults and children from 3 years of age for the prevention of
influenza disease caused by the two influenza A virus subtypes and the two influenza B virus types
contained in the vaccine. Dosage and administration: Adults: 0.5 ml (0.5ml = 1 dose). Paediatric
population: Children from 36 months onwards: 0.5 ml. For children aged < 9 years, who have not
previously been vaccinated, a second dose should be given after an interval of at least 4 weeks. Children
less than 3 years: the safety and efficacy of Fluarix Tetra in children less than 3 years have not been
established. Immunisation should be carried out by intramuscular injection. Contraindications:
Hypersensitivity to the active substances, to any of the excipients or to any component that may be
present as traces such as eggs (ovalbumin, chicken proteins), formaldehyde, gentamicin sulphate and
sodium deoxycholate. Immunisation shall be postponed in patients with febrile illness or acute infection.
Special precautions and special warnings: It is good clinical practice to precede vaccination by a
review of the medical history (especially with regard to previous vaccination and possible occurrence of
undesirable events) and a clinical examination. As with all injectable vaccines, appropriate medical
treatment and supervision should always be readily available in case of an anaphylactic event following the
administration of the vaccine. Antibody response in patients with endogenous or iatrogenic
immunosuppression may be insufficient. Fluarix Tetra is not effective against all possible strains of
influenza virus. Fluarix Tetra is intended to provide protection against those strains of virus from which the
vaccine is prepared and to closely related strains. As with any vaccine, a protective immune response may
not be elicited in all vaccinees. Fluarix Tetra should under no circumstances be administered
intravascularly. As with other vaccines administered intramuscularly, Fluarix Tetra should be given with
caution to individuals with thrombocytopenia or any coagulation disorder since bleeding may occur
following an intramuscular administration to these subjects. Syncope (fainting) can occur following, or even
before, any vaccination especially in adolescents as a psychogenic response to the needle injection. This
can be accompanied by several neurological signs such as transient visual disturbance, paraesthesia and
tonic-clonic limb movements during recovery. It is important that procedures are in place to avoid injury
from faints. Interaction with other medicinal products and other forms of interaction: No interaction
studies have been performed. If Fluarix Tetra is to be given at the same time as another injectable
vaccine, the vaccines should always be administered at different injection sites. Following influenza
vaccination, false positive results in serology tests using the ELISA method to detect antibodies against
HIV1, Hepatitis C and especially HTLV1 have been observed. The Western Blot technique disproves the
false-positive ELISA test results. The transient false positive reactions could be due to the IgM response
by the vaccine. Pregnancy/lactation: Inactivated influenza vaccines can be used in all stages of
pregnancy. Larger datasets on safety are available for the second and third trimester, compared with the
first trimester; however, data from worldwide use of inactivated influenza vaccines do not indicate any
adverse foetal and maternal outcomes attributable to the vaccine. Fluarix Tetra may be used during
breastfeeding. Undesirable effects reported in clinical trials: See SPC for full details. Very common:
irritability, myalgia, injection site pain, fatigue. Common: appetite loss, drowsiness, headache,
gastrointestinal symptoms (including nausea, vomiting, diarrhoea and/or abdominal pain), arthralgia,
injection site redness, injection site swelling, shivering, fever Uncommon: dizziness, rash, injection site
hematoma, injection site pruritus. In addition, the following adverse reactions were reported in previous
Fluarix trials: Common: sweating, injection site induration. Undesirable effects reported during post
marketing surveillance: There has been no post-marketing exposure to Fluarix Tetra. However, as all
three of the influenza strains contained in Fluarix™ are included in Fluarix Tetra, the following adverse
events that have been observed for Fluarix™ during post-marketing surveillance may occur in patients
receiving Fluarix Tetra post-approval. Rare: transient lymphadenopathy, allergic reactions (including
anaphylactic reactions), urticaria, pruritus, erythema, angioedema, influenza-like illness, malaise, neuritis,
acute disseminated encephalomyelitis, Guillain-Barré syndrome. Spontaneous reports of Guillain-Barré
syndrome have been received following vaccination with Fluarix; however, a causal association between
vaccination and Guillain-Barré syndrome has not been established. Overdose: Overdosage is unlikely to
have any untoward effect. Legal category: POM. Presentation: 0.5 ml suspension in prefilled syringe
(Type I glass) with a plunger stopper (grey butyl rubber) with or without fixed needle – pack size of 1 or
10.Special precautions for storage: Store in a refrigerator (2 °C – 8 °C). Do not freeze. Store in the
original package in order to protect from light. MA numbers : Czech Republic: 59/145/14-C Germany:
PEI.H.11629.01.1; Belgium: BE456924; Spain: 78.568; Switzerland: 62961 (Swissmedic), Turkey:
2014/200 USA: US License 1617
Please consult the full Prescribing Information approved in your country.
Procedure for reporting of adverse events:
Adverse events should be reported, please refer to your local national
pharmacovigilance procedure. Adverse events should also be reported to
GlaxoSmithKline on 0800 221 441 in the UK or 1800 244 255 in Ireland
Belgium: Federal Agency for Medicines and Health Products (FAMHP), Belgian
Centre for Pharmacovigilance for medicines for Human use (BCPH), Eurostation II
Place Victor Horta 40/40, B-1060 Brussels Website: www.fichejaune.be
Czech Repubiic: Státní ústav pro kontrolu léčiv Šrobárova 48 100 41 Praha 10,
Webové stránky: www.sukl.cz/nahlasit-nezadouci-ucinek
France: Agence nationale de sécurité du médicament et des produits de santé
(Ansm) et réseau des Centres Régionaux de Pharmacovigilance Site internet:
www.ansm.sante.fr
Italy: Agenzia Italiana del Farmaco Sito web:
http://www.agenziafarmaco.gov.it/it/responsabili
Spain: Spanish Pharmacovigilance System for Medicinal Products for Human Use
(SEFV-H) Website: https://www.notificaram.es/
Switzerland: Please report any adverse event at [email protected]
Turkey: Turkish Pharmacovigilance Center (TUFAM), ankiri Cd. No:57 06060
Diskapi/ANKARA. Website: http://www.iegm.gov.tr/
Germany: Bundesinstitut für Impfstoffe und biomedizinische Arzneimittel, PaulEhrlich-Institut, Paul-Ehrlich-Str. 51-59, 63225 Langen, Tel: +49 6103 77 0, Fax: +49
6103 77 1234, Website: www.pei.de
USA: GlaxoSmithKline: Tel: 1-888-825-5249 or VAERS: Tel: 1-800-822-7967 or
Website: www.vaers.hhs.gov.
For Australia, Hong Kong/Macau and Taiwan only
Highlights of prescribing Information – Refer to full SmPC before prescribing.
NAME OF THE MEDICINE
Fluarix Tetra influenza vaccine (split virion, inactivated)
DESCRIPTION
Fluarix Tetra is an inactivated and purified split influenza vaccine. The antigen
composition and strains for the 2014 influenza season corresponds to the following types:
A/California/7/2009 (H1N1)pdm09-like virus
A/Texas/50/2012 (H3N2)-like virus
B/Massachusetts/2/2012-like virus
The vaccine presents as a colourless to slightly opalescent suspension.
The syringe should be shaken and inspected visually for any foreign particulate matter and/or
variation of physical aspect prior to administration. In the event of either being observed, discard
the vaccine.
Any unused product of waste material should be disposed of in accordance with local
requirements.
Fluarix Tetra is for single use in one patient only.
OVERDOSAGE
Insufficient data are available.
PRESENTATION AND STORAGE CONDITIONS
Fluarix Tetra is presented in pre-filled syringes as pack sizes of 1 or 10.
MA Nos. Australia: PM-2012-02287-3-2; Hong Kong/Macau: HK62235; Taiwan No. 000939
B/Brisbane/60/2008-like virus
Fluarix Tetra is prepared using whole virus cultivated in embryonated hens' eggs. The virus is
concentrated and purified by clarification, adsorption and centrifugation. The purified whole virus
is then treated with the detergent sodium deoxycholate and again centrifuged, and the resulting
antigen suspension is inactivated with formaldehyde.
Suspension for injection.
Fluarix Tetra is a colourless to slightly opalescent suspension.
INDICATIONS
Fluarix Tetra is a quadrivalent vaccine indicated for active immunisation of adults and
children from 3 years of age for the prevention of influenza disease caused by the
influenza virus types A and B contained in the vaccine.
The use of Fluarix Tetra should be based on official recommendations
CONTRAINDICATIONS
Fluarix Tetra should not be administered to individuals with known hypersensitivity after
previous administration of Fluarix Tetra or influenza vaccines or to any component of the vaccine.
PRECAUTIONS
Fluarix Tetra should under no circumstances be administered intravascularly.
As with all injectable vaccines, appropriate medical treatment and supervision should always be
readily available in case of an anaphylactic event following the administration of the vaccine.
As with other vaccines, vaccination with Fluarix Tetra should be postponed in individuals suffering
from an acute severe febrile illness. The presence of a minor infection, such as a cold, should not
result in the deferral of vaccination.
It may be expected that in patients receiving immunosuppressive treatment or patients with
immunodeficiency, an adequate immune response may not be elicited.
Fluarix Tetra is not effective against all possible strains of influenza virus. Fluarix Tetra is intended
to provide protection against those strains of virus from which the vaccine is prepared and to
closely related strains.
Patients with a history of Guillain-Barre Syndrome (GBS) with an onset within six weeks of an
influenza vaccination may be at increased risk of again developing GBS
if given influenza vaccine. Such risk should be weighed against the benefits to the individual
patient of influenza vaccination.
DOSAGE AND ADMINISTRATION
Fluarix Tetra should under no circumstances be administered intravascularly.
Dosage
Fluarix Tetra should be administered as a single 0.5 ml injection.
Children 3 years to less than 9 years of age who have not previously been vaccinated against
influenza should receive a second dose of 0.5 ml after an interval of at least 4 weeks.
Administration
Vaccination should be carried out by intramuscular injection preferably into the deltoid muscle or
anterolateral thigh (depending on the muscle mass).
Instructions for use and handling
Procedure for reporting of adverse events:
Adverse events should be reported, please refer to your local national pharmacovigilance
procedure. Adverse events should also be reported to GlaxoSmithKline on 0800 221 441 in
the UK or 1800 244 255 in Ireland
Australia: Health professionals, manufacturers and sponsors call the TGA on 1800 044 114 or
email [email protected] Sponsors and manufacturers can also email reports
to [email protected] (ICHE2B formatted reports only)
Hong Kong: Fill out online ADR report form at:
http://www.drugoffice.gov.hk/eps/do/en/healthcare_providers/adr_reporting/adr_report_form_elec
tronic.html; or download an ADR report form (available at
http://www.drugoffice.gov.hk/eps/do/en/healthcare_providers/adr_reporting/adr_report_form.html
and return the completed report by: mail using the self-addressed ADR report form or send to the
Pharmacovigilance Unit, Drug Office, Department of Health at Room 1856, Wu Chung House,
213 Queen's Road East, Wanchai, Hong Kong; or fax to 2186 9845; or email to [email protected].
Taiwan: Please fill the Post-marketing ADR Reporting Form to expedite the ADR reporting. All
ADR reports can be sent to the National ADR Reporting Center by facsimile (Fax: 886-2-23584100), postal mail (Mail address: National ADR Reporting Center 2F, No.32, Roosevelt Rd.,
Taipei , 100, Taiwan ), and email ([email protected]) or simply submit on-line through ADR
website. (http://adr.doh.gov.tw/default.asp )
Macau: Contact the China Food and Drug Administration; Address: 26 Xuanwumen Xidajie,
Beijing, 100053, P.R. China