Antonio Frassoldati – Oncologia Ferrara
Il carcinoma mammario
• Epidemiologia e Fattori di rischio
• Diagnosi
– Screening
– Sintomi e segni clinici
• Mammografia ed ecografia
• Citologia e microistologia
• Stadiazione
• La terapia
– Chirurgica
– Radiante
– Medica
• La strategia terapeutica
– Terapia primaria o neo-adiuvante
– Terapia adiuvante
– Terapia della fase metastatica
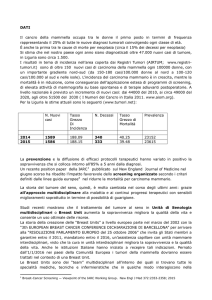
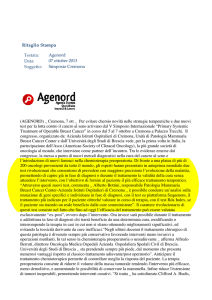
Female cancer statistics
Estimated incidence
Estimated deaths
Brain & other nervous system
Melanoma of skin
3%
2%
Thyroid
2%
15%
Breast
Breast
30%
25%
Lung & bronchus
Lung & bronchus
12%
5%
Pancreas
Pancreas
2%
2%
Stomach
Colon & rectum
11%
11%
Ovary
4%
5%
Ovary
Uterine corpus
6%
2%
Uterine corpus
Urinary bladder
2%
5%
Non-Hodgkin’s lymphoma
Non-Hodgkin’s lymphoma
4%
4%
Leukemia
All others
22%
2%
Multiple myeloma
21%
Colon & rectum
All others
Adapted from Greenlee RT, et al. CA Cancer J Clin. 2000;50:16.
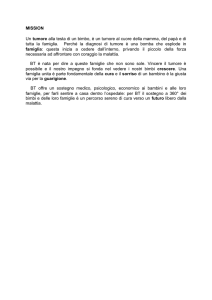
Probabilità del carcinoma mammario
Rischio accumulato per fasce d’età
Età di 30
1 su 2525 donne
Età di 40
1 su 217 donne
Età di 50
1 su 50 donne
Età di 60
1 su 24 donne
Età di 70
1 su 14 donne
Età di 80
1 su 10 donne
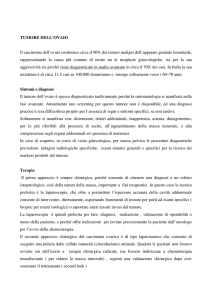
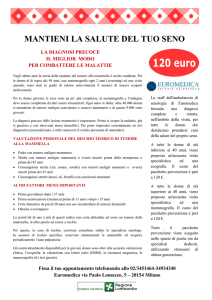
Incidenza per fasce d’età
Carcinoma del seno, tasso standardizzato per età e popolazione mondiale,
sesso femminile, 1988-1993
450
400
350
America del nord
Europa
Mondo
300
250
200
Asia centrale
Asia sud-est
150
100
50
0
15-44
45-54
55-64
65+
EPIDEMIOLOGIA
IN EMILIA-ROMAGNA
•
•
•
•
Oltre 3.300 nuovi casi/anno (dal 1995)
163,5 ogni 100.000 donne residenti
29% di tutti i nuovi casi di tumore nelle donne.
Il 46,5% dei tumori della mammella è
compreso nella fascia di età coinvolta nel
programma di screening (50-69 anni).
• In Italia, nell'analogo periodo, i nuovi casi/anno sono
stati circa 27.500: il 27% di tutti i nuovi casi di
tumore nelle donne.
Incidenza e Mortalità per carcinoma
mammario nella Provincia di Modena
Anno 2002
Anno 2003
Incidenza
Mortalità
Incidenza
Mortalità
Numero casi
556
151
581
110
Tasso grezzo
169
45,9
174,7
33,1
Tasso
standardizzato
Italia
134,9
32,1
135,8
22,8
Tasso
standardizzato
Europa
129,3
28,6
128,9
20,1
Tasso Grezzo: rapporto fra numero casi e popolazione in esame
Tasso standardizzato: rapporto fra numero di casi e popolazione ideale
(Ita/Eur) se i tassi fossero quelli della popolazione studiata
Dati Registro Tumori Provincia di Modena
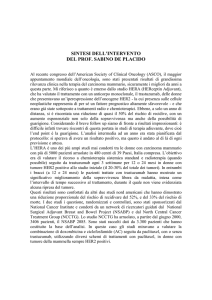
Pazienti con carcinoma mammario seguiti
presso il Dipartimento di Oncologia ed
Ematologia dell’Università di Modena
1600
N. PAZIENTI
1400
1200
1000
2003
2004
2005*
800
600
400
200
0
Mal Locale
* 2005: PRIMI 9 MESI
Mal Avanzata
Totale
Sopravvivenza e Mortalità
• Sopravvivenza
– Italia:
• 74% per gli anni 1990-1994 (a 5 anni)
• 70% nel periodo 1986-1989
– Emilia-Romagna:
• 82 a 84%.
• Mortalità sostanzialmente stabile
– 38 x 100.000, con sostanziale differenza fra aree
geografiche (diversa diffusione delle attività di diagnosi
precoce)
– Italia: (1997), sono morte 11.339 donne per tumore della
mammella (17,3% di tutti i decessi per tumore nella donna)
– Emilia-Romagna: (1999) sono decedute 979 per tumore
della mammella (il 16,3% di tutti i decessi per tumore) .
Breast cancer mortality reduction since 1950
EBCTCG, Lancet 2005
INCIDENZA E MORTALITA’
TREND TEMPORALI
Dati Registro Tumori Provincia di Modena, 2003
SOPRAVVIVENZA
IN PROVINCIA DI MODENA
Dati Registro Tumori Provincia di Modena, 2003
Fattori di rischio
Età
Anamnesi familiare
BRCA1/BRCA2
Cultura occidentale
Radiazioni ionizzanti
Precedenti tumori
Mastopatia fibrocistica
Mestruazioni precoci
Prima gravidanza
Mancanza di figli
Menopausa
Alcool
Celibi/sposati
Zone urbane/rurali
Apporto di grassi
Obesità (postmenopausa)
Attività fisica
Fattore di rischio
>60
Parentela di primo rango
Rischio relativo
4-5
2-4
30
2-3
1-?
Colon, utero, ovaie e seno
<12
>30
1.1-2
1.1-2
1.1-2
>55
1.1-2
> 2 drink/day
1.1-2
1.1-2
1.1-2
>38 % di calorie di grassi 1.1-2
>90 percentile
1.1-2
bassa
1.1-1.5
Il carcinoma mammario
• Epidemiologia e Fattori di rischio
• Diagnosi
– Screening
– Sintomi e segni clinici
• Mammografia ed ecografia
• Citologia e microistologia
• Stadiazione
• La terapia
– Chirurgica
– Radiante
– Medica
• La strategia terapeutica
– Terapia primaria o neo-adiuvante
– Terapia adiuvante
– Terapia della fase metastatica
TUMORI RISCONTRATI NEL PROGRAMMA DI
SCREEENING IN EMILIA ROMAGNA
Stadio
0
Stadio
I
Stadio
II
Stadio
III-IV
Scono
sciuto
Totale
Stadi
≥II
(%)
I
317
1.296
ROUND (13,6%) (55,7%)
587
(25,2%)
56
(2,4%)
72
(3,1%)
2.328
28,5
II
294
1.079
ROUND (15,4%) (56,5%)
452
(23,7%)
32
(1,7%)
52
(2,7%)
1.909
26,1
III
120
420
ROUND (14,7%) (51,6%)
225
(27,7%)
13
(1,6%)
36
(4,4%)
814
30,6
• Rispetto all’era pre-screening, oltre il 20% delle neoplasie
invasive è stato diagnosticato in fase piu’ precoce.
• La percentuale di casi in stadio avanzato (≥II) rimane ancora
attestata al di sopra degli standard consigliati.
RISULTATI DEGLI STUDI
RANDOMIZZATI
Numero di donne da
Rischio
Riduzione
invitare per prevenire
Relativo di
assoluta del
morte per Ca rischio, x1000 una morte 13-20 anni
dopo la
mammario
donne
randomizzazione
Stoccolma
(40-64 aa)
0,91
0,28
3448
Goteborg
(39-59 aa)
0,76
0,87
1139
Malmo
(45-70 aa)
0,82
1,71
584
Swedish Two
County
(40-74 aa)
0,68
1,8
553
Humphrey, Ann Int Med 2002
Breast Imaging
•
•
•
•
•
•
Mammography
US
+ Clinical examination
Magnetic Resonance
Interventistic techniques
TC
Nuclear Medicine
Breast Imaging
Mammography
gold standard
Advantages
Limitations
• Good sensitivity
• Low specificity
• Panoramic view
• Dense breast
• Identification of
microcalcifications
• Breast feeding
• Relative safe
• Quick execution
• Breast implants
Fat breast
Mixed breast
Dense breast
Symptomatic
patient
Where is the
cancer?
Breast Imaging
Sonography - Advantages
• Study of radiologically dense breast
• Tumor size
• Color – doppler
• Axillary involvement
• Guide to interventistic techniques
• Study of breast in pregnancy and breast
feeding
• Study
of breast implant
MRI Identifies More Incidental
Lesions (IL) Than Mammography:
IBMC 6883 study
MRI
Mammography
Patients with
≥ 1 IL identified
129
41
Patients with
suspicious IL
103
36
78
20
56
17
Patients with suspicious
IL confirmed by biopsy
Patients with
cancerous IL
Schnall MD, et al. 40th ASCO; June 5-8, 2004; New Orleans, Louisiana. Abstract 504.
MRI effectiveness in early
breast cancer diagnosis
195 women at high risk due to BRCA1 or BRCA2 carrier
Exam
Diagnostic yeld (%)
Additional cancer
Yeld (%)
Mx
2 (1.2%)
0 (0%)
US
1 (0.6%)
0 (0%)
MRI
6 (3.5%)
4 (2.3%)
MINIMALLY INVASIVE
BREAST BIOPSY
ANATOMIA DELLA MAMMELLA
ORIGINE E SVILUPPO DEL
CARCINOMA MAMMARIO
CLASSIFICAZIONE DEI TUMORI
MAMMARI
• Neoplasie in situ
– duttale (DIN)
– lobulare (LIN): non è considerata lesione tumorale
• Carcinomi invasivi
–
–
–
–
–
–
–
Duttale
Lobulare
Midollare
Apocrino
Papillare
Mucinoso: buona prognosi
Tubulare: buona prognosi
Il carcinoma mammario
• Epidemiologia e Fattori di rischio
• Diagnosi
– Screening
– Sintomi e segni clinici
• Mammografia ed ecografia
• Citologia e microistologia
• Stadiazione
• La terapia
– Chirurgica
– Radiante
– Medica
• La strategia terapeutica
– Terapia primaria o neo-adiuvante
– Terapia adiuvante
– Terapia della fase metastatica
STADIAZIONE
STADIAZIONE
STADIAZIONE
pT1
pN0
pT2
pN0i+
pT3
pN1m
pT4a
pN2
pT4b
pN3
pT4c
pT4d
M0
M1
Crescita e diffusione dei tumori
TRANSFORMATION
ADHERENCE
MOTILITY & INVASION
ANGIOGENESIS
ARREST IN
CAPILLARY BEDS
Capillaries,
Venules, Lymnphatics
EMBOLISM &
CIRCULATION
TRANSPORT
Multicell aggregates
(Lymphocyte, platelets)
EXTRAVASATION
INTO ORGAN
PARENCHYMA
RESPONSE TO
MICROENVIRONMENT
METASTASES
METASTASIS OF
METASTASES
TUMOR CELL
PROLIFERATION
& ANGIOGENESIS
DIFFUSIONE DEL CM
Indagini di stadiazione
• Locale
– Mammografia, ecografia
– Esame clinico
• Generale
–
–
–
–
Rx torace
Ecografia epatica
Scintigrafia ossea
Esami bioumorali (emocromo, fosf.alcalina, Ca, LDH,
transaminasi)
• Esami complementari
– ECG ed Ecocardiogramma
TUMORE DELLA MAMMELLA
STADIAZIONE
La dimensione del
tumore (T), lo stato
linfonodale (N) e la
diffusione metastatica a
distanza (M)
definiscono lo stadio
TNM del tumore
la sopravvivenza è
correlata allo stadio
T1N0M0 (st.I) 87% a 5 aa
ogniT,ogniN,M1 (St. IV)
10% a 5 aa
Il carcinoma mammario
• Epidemiologia e Fattori di rischio
• Diagnosi
– Screening
– Sintomi e segni clinici
• Mammografia ed ecografia
• Citologia e microistologia
• Stadiazione
• La terapia
– Chirurgica
– Radiante
– Medica
• La strategia terapeutica
– Terapia primaria o neo-adiuvante
– Terapia adiuvante
– Terapia della fase metastatica
Chirurgia
• Mammella
– Mastectomia
• Radicale, allargata, modificata
– Quadrantectomia
– Tumorectomia
– Chirurgia ricostruttiva
• Ascella
– Svuotamento ascellare
– Biopsia linfonodo sentinella
PROTESI PER RICOSTRUZIONE
Breast Reconstruction with Expander + Implants
Complicanze chirurgiche
• Emorragie e deiescenza della ferita
• Asimmetrie ed inestetismi
• Dolore alla spalla e disestesie
• Scapola alata e disfunzioni motorie
• Linfedema
Radioterapia
• La radioterapia fa parte dei trattamenti
locali del tumore mammario
• Deve essere eseguita in tutti i casi di
quadrantectomia, o quando la estensione
locale della malattia renda elevato il
rischio di recidiva
• Nella malattia metastatica viene eseguita
con finalità palliative (controllo del dolore o
prevenzione fratture)
OBBIETTIVI
DEL TRATTAMENTO MEDICO
• Terapia primaria
– Conservazione mammaria ed ascellare
– Tasso di risposte complete patologiche
• Terapia adiuvante
– Riduzione della mortalità specifica
– Riduzione del tasso di recidive
• Terapia della fase avanzata
–
–
–
–
Prolungamento della sopravvivenza
Prolungamento del tempo a progressione
Risposta clinica
Controllo dei sintomi
OBBIETTIVI DELLA TERAPIA NELLA
MALATTIA METASTATICA
Characteristics
Objectives
Treatment options
Symptomatic/
poor OS
Palliation
Low toxic CT
Elderly / indolent
disease / poor OS
Improve TTP
& QoL
Low toxic CT / OT
Amenable to
locoregional control
Increase RR
Upfront aggressive
combinations
Young / good PS
/ visceral mets
Prolong survival
Upfront aggressive
combinations
• Oligometastatic disease (1-3% of
Is “cure” a possible
endpoint ?
Few reports with adequate follow-up!
MBC patients)
• Multidisciplinary approach
(surgery, (HD)CT, RT)
• 5-10-15 year survival: 36%, 26%,
24% (vs 7, 4, 3% for historical controls)
• Young, good PS, ER+, Her2 –,
limited disease (candidate to
“palliative” approach)
• Does 20-year DFS represent cure?
Level III and II evidence!
• Selected patients can be
1581
women
treated at
approached
with
a “curative”
intent
MDACC, with doxorubicin
• Intensivecontaining
follow-upchemotherapy
could be
revisited
(Cancer, 1999; 85:104-11)
• Search for parameters really
predictive of long-term survival
RIDUZIONE DELLA MORTALITA’ CON
CHEMIOTERAPIA NELLA MALATTIA
METASTATICA
No of
patients
Odd ratio
response
death
Poly / single
2,442
1.79*
0.82*
Anthra / no anthra
5,241
1.30*
0.96
Taxanes / no taxanes
3,643
1.29*
0.90*
Comparison
HR
* Significant difference
Ghersi D et al., The Cochrane Library, 2003
Fossati. JCO 1998
IMPATTO DEI NUOVI FARMACI SUL
MIGLIORAMENTO OTTENUTO
Multivariate analysis
(2151 MBC patients)
I (91–92)
II (94–95)
III (97–98)
IV (99–01)
I baseline
II paclitaxel, navelbine
III docetaxel, NsAI
IV trastuzumab, capecitabine
HR
of death
1.00
0.97
0.84
0.71
p-value
–
0.65
0.011
<0.001
Chia SLK, et al., ASCO 2003
Can Response rate be improved?
70
60
50
Her-based
40
%
Tax-based
30
Anthra-based
20
10
Pre-Anthra
0
Mean values from pooled studies
ARE IMPROVEMENTS IN RESPONSE RATE USEFULL ?
CT
RR % (CR)
TTP mos
OS mos
Chan ’99
T vs A
48 vs 33*
26 vs 21
15 vs 14
Paridaens’00
P vs A
25 vs 41
7.5 vs 3.9
18.3 vs 15.6
Bishop’99
P vs CMFP
29 vs 35 (2/6)
5.3 vs 6.4
17.3 vs 13.9*
Nabholtz’01
AT vs AC
59 vs 47* (10/7)
9.3 vs 7.9*
22.5 vs 21.7
Nabholtz’02
TAC vs FAC
54 vs 43*
NA
NA
Jassem’01
AP vs FAC
68 vs 55* (19/8)
8.3 vs 6.2*
23.3 vs 18.3*
Biganzoli’02
AP vs AC
58 vs 54 (7/3)
6 vs 6
20.6 vs 20.5
Luck’01
EP vs EC
46 vs 41
9.8 vs 8
18.3 vs 22
* p < 0.005
RISPOSTA DEL TUMORE E
PALLIAZIONE DEI SINTOMI
100
75
Pts with
improvement
%
50
25
ia
An
or
ex
a
N
au
se
t.
ns
De
pr
es
Co
si
on
B
So
Pa
Data base: National
Cancer Institute of
Canada Clinical Trial
Group MA-8 - 300 pts
in
0
CR/PR
SD
PD
Geels et al: JCO 2000; 18: 2395-2405
UN AUMENTO DI SOPRAVVIVENZA DI 3
MESI E’ CONSIDERATO UN BENEFICIO?
60
50
40
Controls
Nurses
General Pract.
Oncologists
Patients
30
20
10
0
1% chance of 3 mos gain in 1% symptom
cure
life
control
Slevin et al. Br Med J 1990; 300: 1458-60
VALUTAZIONE DELLA
QUALITA’ DI VITA
QLQ-30
Global health
status
Function:
Physical
Role
Emotional
Cognitive
Social
SEIQoL*
Nausea/vomiting
Family
Fatigue
Pain
Health
Social life
Dispnoea
Insomnia
Spiritual life
Friendship
Anorexia
Stipsis
Work
Finances
Diarroea
Financial problem
Marriage
Mobility
Pain Free
*Schedule for the Evaluation of Individual Quality of Life, Waldron et al JCO 199; 17: 3603-11
Primary/Neoadjuvant Chemotherapy:
Potential Advantages
•
•
•
•
Early initiation of systemic therapy
Inhibition of post-surgical growth spurt
Provides in vivo anti-tumor assessment
Improved Tumor Downstaging
– Inoperable
Operable
– Mastectomy
BCT
– Improves the rate of breast conservation
surgery
• Provides opportunity to assess surrogate
biological endpoints
INCREMENTO DELLE RISPOSTE
PATOLOGICHE COMPLETE CON
CHEMIOTERAPIA PRE-OPERATORIA
70,0
60,0
pCR %
65.2
50,0
40,0
30,0
30.8
20,0
10,0
0,0
18.9
9.8
B18
22.4
22
15.4
9.8
B27
26.3
ECTO
w/o Tax
Tax301
11.5
GeparDuo MDACC*
w Tax
* With Tax and Trastuzumab, in HER2 3+ only pts
Perché serve una terapia dopo
la asportazione del tumore ?
E’ una terapia
precauzionale, per
distruggere la malattia
microscopica ed evitare
la ricomparsa della
malattia
Quali sono le terapie con farmaci
usate nel carcinoma mammario?
• Chemioterapia
• Terapia ormonale
• Terapia targeted (biologica, a bersaglio
molecolare)
Come funzionano queste terapie?
v Colpiscono i meccanismi
con cui le cellule si
moltiplicano e ne
provocano la distruzione
v Bloccano la produzione
di sostanze che
stimolano la crescita
delle cellule tumorali
v Stimolano i meccanismi
di difesa dell’organismo
RIDUZIONE DI MORTALITA’ E
RECIDIVA CON TERAPIA ADIUVANTE
Comparison (N)
% Risk reduction in
Recurrence
Death
CMF vs. Nil (26,000 < 50)
+41
+34
CMF+ vs. Nil (62,000 50+)
+19
+10
ADM+ vs CMF (25,000)
+6
+9
EPI+ vs. CMF (8,800)
+3
+7
FAC vs. CMF (22,000)
+17
+25
FEC vs CMF (12,000)
+19
+26
CT/Tam vs. Tam (15,000 <50)
+35
+34
CT/Tam vs. Tam (72,000 50+)
+16
+10
(Lancet 2005)
Miglioramento della sopravvivenza con
antracicline in adiuvante
Absolute reduction at 10 years
Relapse
Death
EBCCTG, Oxford 2000
Miglioramento della sopravvivenza con taxani
in adiuvante
Improved outcomes from
adding sequential
Paclitaxel but not from
escalating Doxorubicin
dose in an adjuvant
chemotherapy regimen for
patients with nodepositive primary breast
cancer.
Henderson et al: JCO 2003
PRINCIPALI TOSSICITA’ DEI
CHEMIOTERAPICI
• Cardiac toxicity
– Anthracyclines, Cyclophosphamide, Ifosfamide,
Fluorouracil, Paclitaxel
• Renal toxicity
– Cisplatin, Ifosfamide, Mytomicin
• Gastro-intestinal toxicity
– Vomiting: Cisplatin, Dacarbazine, Mecloretamine,
Anthracyclines
– Dhiarrea: Fluorouracil, Irinotecan
• Neurological toxicity
– Vinca alcaloids, Paclitaxel, Cisplatin, Cytosine
arabinoside
PRINCIPALI TOSSICITA’ DEI
CHEMIOTERAPICI
Timing
– Immediate
• Allergic, Gastrointestinal, Cardiac
– Delayed
• Gastrointestinal, Renal, Hematological,
Neurological, Mucosal
– Late
• Cardiac, Respiratory, Gonadal, Neoplastic
EFFETTI COLLATERALI A BREVE TERMINE
FAC
AC-T
TAC
DD-ACT
ANC
49.3
62-16
65.5°
3 - 9
Febrile
neutropenia
Peripheral
neurotox
Mucositis
2.5
17-11*
24.7°
2
0
3
n.r.
2.0
10-1**
7.1
1.9 –
4.5
5
Vomiting
7.3
27-1**
4.3
8
° 20 and 3.5% respectively in GEICAM 9805 study, with prophylactic G-CSF
* Figures refer to the AC and the Tax Phases. G2-4 side effects
** G1-4 side effects
EFFETTI COLLATERALI A
LUNGO TERMINE
Leukemia
- MDS
Cardiac
toxicity
Anthrabased
0.2-0.6
2
Paclitaxel Docetaxel - based
based
0.4-0.5
0.001
0.06-2
1.2
Cognitive impairment: 61% of pts show a decline
after FAC. No data with paclitaxel or
Docetaxel
Il carcinoma mammario
• La chemioterapia
– Modalità di somministrazione
– Indicazioni
– Farmaci utilizzati: meccanismo d’azione
ed efficacia
– Effetti indesiderati
• La terapia ormonale
– Indicazioni
– I farmaci disponibili: meccanismo
d’azione ed efficacia
– Effetti indesiderati
• Le terapia a bersaglio molecolare
– Trastuzumab (Herceptin)
– Bevacizumab (Avastin)
• Le terapie comlpementari
– I difosfonati
MECCANISMO D’AZIONE DELLA
CHEMIOTERAPIA
Antibiotics
Antimetabolites
S
(2-6h)
G2
(2-32h)
M
(0.5-2h)
Vinca alkaloids
Mitotic inhibitors
Taxoids
Alkylating agents
Cell cycle level
G1
(2-∞h)
G0
MECCANISMO D’AZIONE DELLA
CHEMIOTERAPIA
DNA synthesis
Antimetabolites
DNA
DNA transcription
Alkylating agents
DNA duplication
Mitosis
Cellular level
Intercalating agents
Spindle poisons
MECCANISMO D’AZIONE DELLA
CHEMIOTERAPIA
PURINE SYNTHESIS
PYRIMIDINE SYNTHESIS
6MERCAPTOPURINE
RIBONUCLEOTIDES
6-THIOGUANINE
METHOTREXATE
DEOXYRIBONUCLEOTIDES
5-FLUOROURACIL
ALKYLATING AGENTS
HYDROXYUREA
ANTIBIOTICS
DNA
CYTARABINE
ETOPOSIDE
RNA
PROTEINS
L-ASPARAGINASE
VINCA ALKALOIDS
ENZYMES
MICROTUBULES
TAXOIDS
Increaseing
Cell Kill
RAPPORTO DOSE-EFFICACIA
Increasing Dose
ETEROGENEITA’ TUMORALE
Normal
Cell
<
Tumoral
Cell
Clonal expansion
of tumoral cells
Heterogeneity of tumoral cell
RESISTENZA ALLA CHEMIOTERAPIA
EXTRACELLULAR
PGP170
INTRACELLULAR
ATP
Drug
ATP
Drug
Plasma
Membrane
Chemioterapia standard
intensa
densa
Cell Number
1012
108
104
100
0
20
40
60
Weeks
EFFETTO DELLA CHEMIOTERAPIA SULLA DISTRUZIONE E
RICRESCITA CELLULARE NEL TUMORE
VARIAZIONI DELLA DOSE
Dose escalation = increased dose-size or total dose
vs
Dose-Intensity or Dose-Rate = total dose/time
vs
ALTE DOSI
Dose-Density = relative term
(only meaningful w/ constant dose-size and cycle #)
vs
TP SETTIMANALI
VALUTAZIONE DI NUOVI FARMACI
IN VITRO
Mechanism of action
IN VIVO
Stage I
Stage II
l Target level
l Maximum tolerated dose
l Spectrum of activity
l Cellular level
l Dose-limiting toxicities
l Schedule dependency
l Efficacy
l Route of administration
l Cross resistance
l Combination therapies
VALUTAZIONE CLINICA DI NUOVI
FARMACI
Study Phase
Objectives
Phase I
l Identify maximum tolerated dose l Small (3-6 patients/dose level)
Phase II
l Define key toxicities
l Various tumor types
l Evaluate tumor response
l Larger than Phase I (10-50
l Determine whether drug
patients/treatment group)
l More uniform disease
characteristics
warrants Phase III study
Phase III
Phase IV
Patient Population
l Compare new treatment with
l Larger than Phase II (100s of
standard
l Support marketing approval
patients/treatment group)
l Same tumor type
l Broader patient pool
l Integrate clinical study experience l Very large cohorts (100s-1000s)
into general clinical practice
l Monitor safety after approval
l Represent general patient
population
Come funziona la terapia ormonale?
v Impedisce ai normali
ormoni femminili di
stimolare le cellule
tumorali ad essi
“sensibili”
vBlocca la produzione degli estrogeni
da parte dell’ovaio o di altri tessuti
TERAPIA ORMONALE
GNRH
GNRH agonists
agonists
(A)
(A) Premenopausal
Premenopausal
(B)
(B) Postmenopausal
Postmenopausal
LH
LH
FSH
FSH
Antiestrogen
Antiestrogen
Breast
carcinoma
Breast
carcinoma
Adrenal
Estrogen
Estrogen
Adapted with permission from
Tellez C, et al. Surg Oncol Clin
North Am. 1995;4:751-777.
GNRH = Gonadotropin-releasing
hormone; LH = Luteinizing hormone;
FSH = Follicle-stimulating hormone.
Antiestrogen
Antiestrogen
Estrogen
Estrogen
Androstenedione
Androstenedione
Aromatase
Aromatase
inhibitor
inhibitor
Ovary
Peripheral
Peripheral
aromatization
aromatization
SERMs (= tamoxifene)
ER: Interazione con Estradiolo
ER: Interazione con Estradiolo
ER:
ER: Interazione
Interazione con
con Tamoxifen
Tamoxifen
Fulvestrant
Selective Estrogen Receptor Down-Regulator
Tamoxifen
Fulvestrant
Inibizione
competitiva del
legame degli
Estrogeni con
RE
Blocco della
dimerizzazione,
destabilizzazione
e degradazione
di RE
Ridotta
trascrizione dei
geni regolati da
RE, compreso
RPg
INIBITORI DELLE AROMATASI
(anastrozolo, letrozolo, examestano)
Antiestrogens
Estrogen
Estrogen
biosynthesis
biosynthesis
Nucleus
Nucleus
Estrogen
Estrogen
biosynthesis
biosynthesis
Inhibition
Inhibition
of
of growth
growth
Aromatase
inhibitors
Tumor
Tumor cell
cell
ER = Estrogen receptor.
Tamoxifen and Aromatase Inhibitors
ATAC
IES
MA17
PATIENTS
6241
4742
5187
FOLLOW UP (MOS)
33.3
30.6
29
DISTANT EVENTS %
340(49)
262(58)
123(54)
AGE (yrs)
64.1
64.2
62
ADJUVANT RT (%)
63
NA
60
ADJUVANT CT(%)
21.5
32.3
46
DFS
2% AT
3 YRS
4.7% AT
3 YRS
2.2% AT
2.4 YRS
MIGLIORAMENTI CON INIBITORI
DELLE AROMATASI
38% risk of recurrence with no adjuvant treatment1
50% risk reduction with tamoxifen1
Further 26% risk
reduction with
anastrozole2
1. EBCTCG. Lancet 1998; 351: 1451-1467
2. ATAC Trialists’ Group. Lancet 2005; 365: 60-62
EFFETTI COLLATERALI DI TAMOXIFENE
ED INIBITORI DELLE AROMATASI
In favour of
tamoxifen
In favour of
anastrozole
Hot flushes
(-5.4%)
(6.6%) MSK disorders
Weight gain*
(-1.8%)
(2.1%)
Fractures
(0.8%)
Vag. bleeding
Fractures of hip,
spine, wrist
(-3.6%)
Vag. discharge (-8.6%)
Endo Ca
ICVA
(-0.4%)
(-1.1%)
VTE
(-1.4%)
DVT
(-0.7%)
-10
-5
0
5
10
Difference between anastrozole and tamoxifen AEs (%)
* proportion with ≥10% gain in body weight from baseline to year 2
ASPETTO RADIOLOGICO DELLE
METASTASI OSSEE
Lytic
Blastic
Mixed
Osteoporosi
• A skeletal disorder characterized by
compromised bone strength predisposing to
an increased risk of fracture.
Normal Bone
Osteoporotic Bone
Osteoporosis Prevention, Diagnosis, and Therapy. NIH Consensus Statement 2000 March 27-29; 17(1): 1-36.
Dempster, DW, et al., JBMR 2000; 15 (1): 20.
EFFETTO DI ZOLEDRONATO SULLA
MASSA OSSEA
None
Baseline
Zoledronic Acid
after 36 months
T-Score (standard deviations)
0
-0,5
-1
-1,5
-2
-2,5
Gnant M et al., SABCS 2004
- 1.4 standard dev.
p<0.0001
Perché queste terapie possono
essere tossiche?
vPerché colpiscono anche le cellule sane
che si moltiplicano (midollo osseo,
mucose della bocca e dell’intestino,
follicoli piliferi, ..)
vPerché hanno una azione specifica in
particolari zone del corpo (centro del
vomito, ovaio, osso, ...)
Perché si usano se sono tossiche?
VANTAGGI
MAGGIORE
PROBABILITA’ DI
EVITARE LA
COMPARSA DEL
TUMORE E DI
AUMENTARE LA
SOPRAVVIVENZA
SVANTAGGI
TOSSICITA’
EFFETTO SU
QUALITA’ DI
VITA
Cosa abbiamo ottenuto?
vUna riduzione delle
riprese di malattia
del 35% - 50%
vUna riduzione della
mortalità del 30%
Come si sceglie la terapia?
Ø In base a parametri legati al tumore
§
§
§
§
Dimensioni, invasione dei linfonodi ascellari
Caratteristiche del tumore
Ormonosensibilità
Fattori specifici di prognosi
(erbB2, invasione vascolare)
Ø In base alle condizioni
della paziente
§ Età, malattie associate
FATTORI PROGNOSTICI E
PREDITTIVI
FATTORE
PROGNOSTICO
• definisce la storia
naturale del tumore
• indipendente dalla
terapia
• correla con OS e DFS
• utile per la
pianificazione
terapeutica
FATTORE
PREDITTIVO
• predice la risposta
al trattamento
Fattore prognostico e
predittivo non sempre
coincidono
CARATTERISTICHE DEI FATTORI
PROGNOSTICI e PREDITTIVI
• Significatività: la variabile ha un
valore non dettato dal caso
• Indipendenza: la variabile mantiene il
proprio valore prognostico/predittivo
indipendentemente da altri fattori
prognostici
• Rilevanza clinica: utile nel pianificare
la strategia terapeutica del paziente
FATTORI PROGNOSTICI E
PREDITTIVI
Legati al paziente
Parametri clinici
(PS,età…)
Predicono la compliance
alla terapia
Legati alla neoplasia
Stadiazione TNM
Grading
Legati al
trattamento
Biomarcatori
fenotipici
Appropriatezza
Competenza
Currently accepted prognostic/predictive
parameters (St. Gallen, 2005)
• Patient
characteristics
• Disease
characteristics
• Biomarkers
Age
Race
Tumor size
Tumor type
Axillary status
Tumor grade
new! Peritum. vascular invasion
Receptor status
new! HER2/neu expression
new! Ki-67 labeling index
TUMORE DELLA MAMMELLA
RECETTORI ORMONALI
Lo stato recettoriale è un fattore prognostico non
indipendente ma risulta strettamente associato al grado
istologico
TUMORE DELLA MAMMELLA
RECETTORI ORMONALI
• lo stato ER è un fattore predittivo
• Le meta-analisi hanno confermato il valore
predittivo dei ER in termini di risposta a
Tamoxifene. La ⇓ di mortalità a 5 aa è stata
del 47% nelle donne con ER o PgR positivi vs
una ⇓ di mortalità a 5 anni del 26% nelle donne i
cui tumori erano ER o PgR negativi
TUMORE DELLA MAMMELLA
DIMENSIONI DEL TUMORE
Il DFS a 5 e 20 aa dopo trattamento iniziale
varia in funzione delle dimensioni del tumore
<10 mm
88%
11-13 mm
14-16 mm
17-22 mm
73%
65%
59%
Rosen PP Surg Clin North Am 1990
TUMORE DELLA MAMMELLA
STATO LINFONODALE
In base alla valutazione
dei linfonodi si dividono
3 classi di rischio con
prognosi
progressivamente
peggiore:
u N0
u N1-3
u N>4
TUMORE DELLA MAMMELLA
GRADO ISTOLOGICO
St.Gallo 2005: Categorie di rischio
Risk Category
Low Risk
Node Negative AND
ER and/or PgR expressed, AND all of the
following features:
pT< 2cm**, AND
Grade 1, AND
LVI absence, AND
HER2 negativity, AND
Age >35 years
* Microinvasive cancer or specific types of tumor phenotypes
(medullary or apocrine, or myoepithelial cancer) presenting as nodenegative disease - ** pT<1 cm low risk irrespective G3 or Age < 35 yrs
St.Gallo 2005: Categorie di rischio
Risk Category
Intermediate Risk
Node Negative
AND at least one of the following features:
pT> 2cm, OR
Grade 2-3, OR
Age <35 years OR
LVI present, OR
HER2 positive
Node-Positive 1-3 AND
HER2 negative
High Risk
Node-positive 4 or more
OR
Any Node-positive AND HER2 positivity
Cosa ci riserva il futuro?
ØUna migliore capacità di capire il
comportamento del tumore, attraverso
nuove tecniche di analisi
ØLa disponibilità di nuovi farmaci
§ A minore tossicità
§ A diverso meccanismo di azione
§ A maggiore specificità di azione
ØLa possibilità di individualizzare le
terapie, per curare la malattia senza
tossicità sull’organismo.
LA FAMIGLIA DEI
RECETTORI HER
EGF
TGFα
Amphiregulin
β-cellulin
HB-EGF
Heregulins
NRG2
NRG3
Heregulins
β-cellulin
Tyrosine
kinase
domain
erbB-1
HER-1
EGFR
erbB-2
HER-2
neu
erbB-3
HER-3
erbB-4
HER-4
VIE DI TRASMISSIONE DEL SEGNALE
NELLA CELLULA NEOPLASTICA
Growth factor
Binding site
Plasma
membrane
Signal
transduction
to nucleus
Cytoplasm
Tyrosine
kinase activity
Nucleus
Gene activation
CELL
DIVISION
Meccanismi
di controllo
della
The HER/erbB
signalling
cellula
tumorale
network
LPA,
thrombin
ET, etc.
TGFα
(1)
EGF
(1)
Epiregulin
(1,4)
Input
layer
1
3
1
2
1
β-cellulin
(1)
2
1
2
HB-EGF
(1,4)
4
2
Amphiregulin
(1)
NRG1
(3,4)
α
β
1
3
4
NRG2
(4)
α β
2
4
NRG3
(4)
4
3
NRG4
(4)
4
Cytokines
3
Ligands
3
Receptor
dimers
Src
Cbl
Signalprocessing
layer
PLCγ
PKC
Shc
Ras-GDP
Shp2
Grb2
GAP
Ras-GTP
Sp1
Output
Apoptosis
layer
PI3K
RAF
MEK
MAPK
Akt
Bad S6K
Myc
Migration
Jun
Fos
Elk
Growth
Nck
Sos
Vav
Grb7
Crk
Jak
Adaptors
and enzymes
Rac
PAK
JNKK
JNK
Egr1
Abl
Stat
Adhesion
Cascades
Transcription
factors
Differentiation
Yarden Y, Sliwkowski M. Nat Rev Mol Cell Biol 2001;2:127–37
Come colpire il bersaglio
MAbs
TKIs
Toxin
conjugates
Antisense
Ligand
Ligand
Ligand
K K
K K
Cell
death
Protein
synthesis
Ligand
K K
Signal
transduction
K K TKI
Signal
transduction
FARMACI A BERSAGLIO
MOLECOLARE IN COMMERCIO
• Drugs targeting cellular receptors
–
–
–
–
–
Tamoxifen (ER)
Trastuzumab (HER2)
Rituximab (CD20R)
Cetuximab (EGFR)
Bevacizumab (VEGFR)
• Drugs targeting tyrosine-kinase
– Gefitinib
– OSI 747
– Imatinib
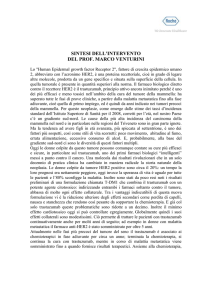
ESPRESSIONE DI HER2
Normal 0
Normal 1+
Abnormal 2+
Abnormal 3+
Normal
Normal
Abnormal low
amplification
Abnormal high
amplification
IHC Images by Kornstein, MD, Medical College of Virginia
Aumento della sopravvivenza con
Herceptin nella malattia metastatica
1.0
0.8
Herceptin + CT
CT alone
0.7
p<0.05
Probability of survival
0.9
®
0.6
0.5
0.4
0.3
0.2
0.1
0.0
20
0
5
10
15
29
20
25
30
35
40
45
50
Time (months)
CT = chemotherapy
Slamon DJ, et al. N Engl J Med 2001;344:783–92
RIDUZIONE DELLE RECIDIVE CON
HERCEPTIN IN ADIUVANTE
B-31/N9831 joint analysis (concurrent)
DFS HR: 0.48 (p= 3x10-12)
HERA trial and N9831 armB (sequential)
DFS HR: 0.54 in the HERA trial (p=<0.00001)
DFS HR: 0.87 in N9831 (p=0.29)
N9831 comparison of concurrent vs sequential
DFS HR: 0.64 (p=0.0114)
BCIRG006 comparison of trastuzumab
combinations with or without anthracyclines
DFS HR for AC-TH: 0.49 (p=<0.0001)
DFS for TCH: 0.61 (p=0.0002)
L’ANGIOGENESI E’ IMPLICATA NELLA
CRESCITA E DIFFUSIONE DEI TUMORI
Premalignant
stage
Malignant
tumour
Tumour
growth
Vascular
invasion
Dormant
micrometastasis
(Avascular
tumour)
(Angiogenic
switch)
(Vascularised
tumour)
(Tumour cell
intravasation)
(Seeding in
distant organs)
Overt
metastasis
(Secondary
angiogenesis)
Stages at which angiogenesis plays a role in tumour progression
Adapted from Poon RT, et al. J Clin Oncol 2001;19:1207–25
AVASTIN NORMALIZZA LA
VASCOLARIZZAZIONE DEL TUMORE
VEGF
Stimulation of vascular permeability
Increased permeability promotes
plasma protein leakage
bevacizumab
Extracellular fibrin
gel formation
Excessive
permeability
results in
uneven delivery
of nutrients and
O2 to
target tissue
Reduces
interstitial fluid pressure
vessel density
Increases
drug delivery
Jain R. Nature Med 2001;7:987–9; Willett CG, et al. Nat Med 2004;10:145–7; Wildiers H, et al. Br J Cancer 2003;88:1979–86
The future of the future
• Tumor diagnosis at preclinical stage
(proteomics)
• Fast, cheap and reproducible characterization
(gene expressio profile) of
– Tumor behavior
– Sensitivity/resistance to specific drugs
– Type of toxicity for each patient
• Minimal surgery and radiation
• Tailored treatment with low toxic drug for a
limited time (Target therapies)
• New hopes for the patients