Considerazioni sulla scelta
antitrombotica della FA nello
scompenso cardiaco
Paolo Colonna, MD FESC FANMCO
Cardiology Hospital, Policlinico of Bari
PROBE
ROCKET AF
14264
73
60
3.5
0
13
87%
55
17.5
62
35.5
38
2.0
0.2
23
New oral anticoagul
in AF
Position del WG
thrombosis ESC
De Caterina,
G It Card 2012
Efficacia: ictus o embolia sist
Guest editor: Paolo Colonna
Sicurezza: emorragie maggiori
Abbiamo paura del “nuovo”
nello scompensato ?
•
•
•
Scompenso cardiaco
Disfunzione renale o epatica
Anziano
Restiamo con il vecchio coumadin?
2
1
cardiac heart failure
EAE recommendations, EJE 2010
AF embolic risk
stratification:
From CHADS2 (2001)
to CHA2DS2VASc (2010)
Echo predictors of stroke in pts with
AF (1066 pts from 3 trials)
AFI invest, Arch Int Med ‘98
Echo predictors of stroke in pts with
AF (1066 pts from 3 trials)
AFI invest, Arch Int Med ‘98
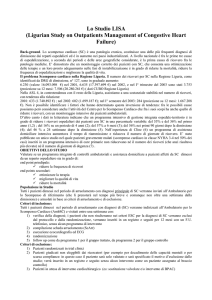
Mechanisms of thrombogenesis in atrial
fibrillation: Virchow's triad revisited
Watson T et al. Lancet 2009
Virchow's triad 1855
Anomalie di:
• parete vaso
• flusso ematico
• componenti
ematiche
Revisited 2009
• micro/macro alteraz
parete LA
• stasi da disfunz LAA
• anomalie emostasi,
piastrine, fibrinolisi
Factors associated with heart failure
predisposing to thrombosis
•
•
•
Vascular pathology
Impaired flow (cardiac and peripheral)
Increased coagulability:
– ↑plasma concentr. of beta-thromboglobulin
(marker platelet activation) and fibrinopeptide A
– thrombin activation
– ↑ plasma concentrations of endothelial
procoagulants, von Willebrand factor,
fibrinolytic products, and D-dimer
Jafri SM. Hypercoagulability in heart failure.
Semin Thromb Hemost 1997;23:543-5.
Causes of death and influencing factors in
AF: a competing risk analysis from ReLY
Marijon, Circulation 2013 in press
With sHF
(n=4904)
Without sHF
(n=13 209)
P value
68.3 (10.2)
72.7 (7.7)
<0.001
Male gender, %
66.9
62.3
<0.001
Diabetes, %
26.5
22.1
<0.001
Hypertension, %
75.2
80.2
<0.001
Stroke, %
10.4
13.3
<0.001
Coronary artery
disease, %
31.8
26.3
0.0003
Valvular H disease, %
26.2
19.8
<0.001
LVEF ≤40%
43.5*
11.2†
<0.001
76.3 (32.6)
71.7 (25.7)
<0.001
RE-LY
Age, yrs, mean (SD)
CrCl, mL/min, (SD)
Type of AF, %
Paroxysmal
Persistent
Permanent
Heart rate, bpm, (SD)
<0.001
21.6
33.9
44.5
37.0
31.2
31.7
76.1 (15.2)
72.6 (14.6)
<0.001
Ferreira et al, EurJHF 2013
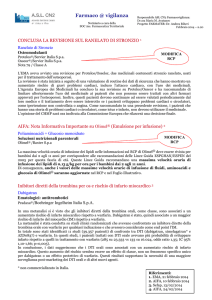
Dabigatran compared with warfarin in AF and
symptomatic heart failure: subgroup of RE-LY
Ferreira et al, EurJHF 2013
Stroke or SE
Rate (% per year)
D110 D150 W
With sHF
1.90
Without sHF 1.41
1.44
D110 vs warfarin
D150 vs warfarin
P (interaction)
P (interaction)
1.92
0.51
1.00
0.39
1.64
0.5
Favours
dabigatran
1.0
1.5
Favours
warfarin
0.5
1.0
Favours
dabigatran
1.5
Favours
warfarin
Dabigatran compared with warfarin in AF and
symptomatic heart failure: subgroup of RE-LY
Ferreira et al, EurJHF 2013
Major bleeding
D110 vs warfarin
Rate (% per year)
D110 D150 W
With sHF
3.26
3.10
D150 vs warfarin
P (interaction)
P (interaction)
3.90
0.74
0.20
Without sHF 2.73
3.39
3.45
0.5
1.0
1.5
0.5
1.0
1.5
Intracranial bleeding
With sHF
0.22
0.26
0.65
0.91
Without sHF 0.23
0.34
0.72
0.80
0 0.5 1.0 1.5 2.0
Favours
Favours
warfarin
dabigatran
0 0.5 1.0 1.5 2.0
Favours
Favours
warfarin
dabigatran
Efficacy and safety of rivaroxaban in
patients with heart failure and AF:
insights from ROCKET AF
Van Diepen et al. CircHF 2013
• Rocket – AF: 63,7% dei pazienti (n=9.033)
con scompenso cardiaco
• mediamente più giovani (72 vs 74 anni),
• più propensi a fibrillazione atriale permanente
(83,0% vs 77,6%)
• punteggi medi CHADS2 più elevati
(3,7 vs 3,1)
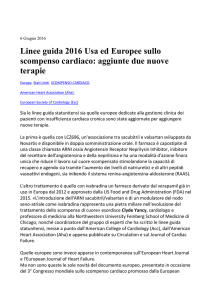
Efficacy and safety of rivaroxaban in
patients with heart failure and AF:
insights from ROCKET AF
Van Diepen et al. Circ H F 2013
Efficacy and safety of rivaroxaban in
patients with heart failure and AF:
insights from ROCKET AF
Van Diepen et al. Circ H F 2013
Nello scompenso cardiaco efficacia di
rivaroxaban simile, indipendente da:
• classe NYHA (New York Class Association)
I-II vs III-IV
• frazione d’eiezione preservata o ridotta
• score CHADS2 2 vs >3
The direct factor Xa inhibitor Rivaroxaban
reduces platelet activation in congestive
heart failure
Flierl U, Pharm Res 2013
Rivaroxaban reduces platelet activation in CHF rats
by attenuating the secondary phase of ADP-induced
platelet aggregation
The direct factor Xa inhibitor Rivaroxaban
reduces platelet activation in congestive
heart failure
Flierl U, Pharm Res 2013
Rivaroxaban prevents thromboembolic
complications and reduce platelet activation in CHF
McMurray et al Circ HF 2013
McMurray Circ HF 2013
McMurray Circ HF 2013
Efficacy and safety of dabigatran etexilate and
warfarin in ‘real world’ patients with atrial fibrillation:
A prospective nationwide cohort study.
Larsen T, et al. JACC 2013
EHRA practical guide on the use of
NOA in patients with atrial fibrillation
Heidbuchel, EHJ 2013
1. Fisiopatologia del tromboembolismo arterioso
2. Stratificazione del rischio di ictus e di
sanguinamento
3. Limiti delle attuali terapie anticoagulanti
4. Trial clinici sui nuovi anticoagulanti orali nella FA
5. Indicazioni e applicazioni pratiche dei NAO
+ costo / efficacia
Fibrillazione atriale e scompenso:
ruolo dei NAO
•
•
FA indica peggior prognosi negli scompensati
Prognosi è intermedia se scompenso a FE
conservata
• Efficacia dei NAO (riduzione ictus ed emorragia)
confermata nei pazienti con scompenso e FA
• Attenzione nei pazienti scompensati, fragili e/o
con disfunzione renale
Abbiamo paura dei
“nuovi arrivati”?
• Dobbiamo prestar “loro” nuove attenzioni
• Dobbiamo conoscere bene i loro lati
“difficili”
... ma ci portano sempre aspetti nuovi e
vantaggiosi