Corso Giovani SIMIT
“Problemi di metodo nelle sperimentazioni cliniche in infettivologia”
Roma, I.N.M.I. “L. Spallanzani”
31 Gennaio – 2 Febbraio 2013
Gli esiti delle sperimentazioni
cliniche
Enrico Girardi
Dipartimento di Epidemiologia
Istituto Nazionale per le Malattie Infettive
Lazzaro Spallanzani - IRCCS , Roma
Come si misurare l'efficacia di un intervento
in una sperimentazione clinica
•Registrare la frequenza di eventi clinicamente
rilevanti nei gruppi inclusi nella sperimentazione
•Questi eventi si definiscono gli esiti della
sperimentazione ( endpoint, outcome)
Clinical endpoint = A measure of how a subject
functions, feel, survive
Esiti di una sperimentazione
clinica
•Morte
•Insorgenza di eventi clinici rilevanti
•Gravità della sintomatologia
•Effetti collaterali
•Qualità della vita
Esiti principali e secondari
Esito principale
•Risponde al quesito centrale della
sperimentazione clinica
•E' l’esito sulla cui frequenza viene condotta
l’analisi principale dello studio
•Lo studio viene dimensionato per rilevare ( se
esiste) un determinata differenza di frequenza
dell'esito principale
Esiti principali e secondari
Esiti secondari
•Forniscono informazioni aggiuntive sugli effetti
dell'intervento studiato valutando altri eventi
clinici o il medesimo evento secondo diversi
criteri
•Lo studio non è dimensionato per rilevare (se
esiste) un determinata differenza di frequenza
degli esiti secondari
•Definiscono ipotesi per studi ad hoc
Antimicrobial catheters for reduction of symptomatic urinary
tract infection in adults requiring short-term catheterisation in
hospital: a multicentre randomised controlled trial
Robert Pickard*,et alLancet 2012; 380: 1927–35
The primary outcome was incidence of symptomatic
CAUTI [ defined as the presence of participant-reported symptoms of
urinary tract infection and clinician prescription of antibiotic for a urinary
tract infection at anytime up to 6 weeks after randomisation]
Secondary outcomes included incidence of
microbiologically confirmed symptomatic CAUTI [which
was defined as the primary outcome and a positive urine culture]; incidence of
bacteriuria up to 3 days after catheter removal;
changes in health-related quality of life during the 6
weeks of trial participation; and urethral discomfort
related to catheterisation.
Antimicrobial catheters for reduction of symptomatic urinary
tract infection in adults requiring short-term catheterisation in
hospital: a multicentre randomised controlled trial
Robert Pickard*,et alLancet 2012; 380: 1927–35
Because a high degree of benefit would be needed to
change routine clinical practice, we specified a 3.3%
absolute reduction on the basis of estimated incidence
in the control group of 11% (30% relative reduction) …
we needed to recruit 2345 participants in each group
(7035 participants overall)
We analysed all included participants in their allocated
group irrespective of the catheter received, according
to intention-to-treat principles, and assumed
participants did not have a symptomatic CAUTI unless
they met the primary outcome criteria.
Esiti di una sperimentazione clinica
Significatività clinica e statistica
Trial clinico Fluvir© (antivirale attivo su virus
influenzale ) vs placebo
Esito rilevato. Durata della febbre
Risultato : pazienti trattati 4,1 giorni – pazienti
controllo 4,8 giorni ; p<0,02
Differenza significativa statisticamente, ma
clinicamente??
Substitution of Moxifloxacin for Isoniazid during
Intensive Phase Treatment of Pulmonary Tuberculosis
Susan E. Dorman Am J Respir Crit Care Med Vol 180. pp 273–280, 2009
The primary efficacy outcome was the percentage of
participants with negative cultures on both liquid and solid
medium at the time of completion of intensive phase (‘‘Week-8
culture negativity’’).
Time to stable culture conversion was a secondary endpoint and
was defined as the number of days from study treatment
initiation to the time of sputum
The primary safety endpoint was permanent discontinuation of
the assigned intensive-phase treatment
Substitution of Moxifloxacin for Isoniazid during
Intensive Phase Treatment of Pulmonary Tuberculosis
Susan E. Dorman Am J Respir Crit Care Med Vol 180. pp 273–280, 2009
Sample size was calculated based on the assumption that
substitution of moxifloxacin for isoniazid would increase the
percentage of participants having negative cultures at the
completion of 8 weeks of treatment by 13%—similar to the
impact of adding pyrazinamide, a drug that allowed overall TB
treatment shortening
Two efficacy analysis groups were prespecified. A modified
intention to-treat (MITT) group excluded participants whose
enrollment specimen failed to grow M. tuberculosis or had
proven resistance… A protocol-correct (PC) group…
For safety analyses, all participants who received at least one
dose of study treatment were included.
Valutare il rischio di effetti avversi gravi
La regola inversa del 3 (D. Sackett)
Per essere sicuri al 95% che un determinato
evento non si verifichi in relazione all’uso di un
farmaco con una frequenza di 1 su x, dobbiamo
studiare 3x pazienti.
Esempio: vogliamo essere sicuri (al 95%) che
una nuova statina non provochi rabdomiolisi
con una frequenza superiore a 1/25.000 pazienti
per anno, dobbiamo seguire per un anno 75.000
(3x25.000) pazienti che assumono questo
farmaco.
Esiti compositi
Diversi eventi clinici sono considerati equivalenti
ai fini del computo della frequenza del’esito
principale
Ad esempio:
AIDS/morte
Ictus ischemico/infarto miocardico/morte
Manifestazioni cliniche da insufficienza
epatica/morte
Costruzione di un esito composito
1. Gli eventi che lo compongono dovrebbero
avere rilevanza clinica paragonabile
2. Gli eventi che lo compongono dovrebbero
avere frequenza paragonabile
3. L’effetto della terapia sul rischio di sviluppare
uno degli eventi che lo compongono
dovrebbe essere simile
3b. Il meccanismo patogenetico alla base degli eventi che lo compongono
dovrebbe essere simile
Irbesartan diabetic nephropaty
trial
Patients with nephropathy and
type 2 diabetes randomized to
to irbesartan, amlodipine, or
placebo.
The primary endpoint was the
composite of a doubling of the
baseline serum creatinine
concentration, the onset of
end-stage renal disease
(serum creatinine > 6.0 mg/dL,
initiation of dialysis, or
transplantation), or death
from any cause.
Esiti surrogati
definizioni
“A validated surrogate endpoint is and endpoint wich
allows the prediction of a clinically important
outcome”
International conference on harmonization - Statement E8
“a laboratory measurement or a physical sign [a
biomarker] used as a substitute for a clinically
meaningful endpoint that measures directly how a
patient feels, functions or survives. Changes induced
by a therapy on a surrogate endpoint are expected to
reflect changes in a clinically meaningful endpoint”
Temple R, JAMA 1999
Quando si usano esiti surrogati?
Nelle patologie croniche
Quando gli esiti clinici rilevanti si verificano in
tempi molto lunghi
Nelgli studi di fase I-II per fornire informazioni
sullo sviluppo potenziale di un farmaco
Biomarcatori –una definizione
“a characteristic that is objectively measured
and evaluated as an indicator of normal
biological processes, pathogenic processes, or
pharmacologic responses to a therapeutic
intervention”
NIH, Biomarkers Working Group
Biomarcatori e endpoint surrogati
Marcatori biologici con valore prognostico sono spesso
potenziali endpoint surrogati
Questo possibile uso va valutato secondo due criteri
1 Criterio causale: l’effetto indotto dalla terapia sul
biomarcatore rispecchia il meccanismo biologico che
determina l’effetto della terapia sul’esito clinico
2 Potere predittivo : l’effetto sul marcatore predice
accuratamente l’effetto sull’esito clinico
Perché un biomarcatore può non
essere un esito surrogato affidabile
Il marcatore è misurato in modo impreciso
Il marcatore non è nella catena causale
dell’evento clinico
Il meccanismo di azione del trattamento non
coinvolge (o coinvolge solo in parte) il
biomarcatore
Il marcatore è misurato in modo
impreciso
Studio iPrEx (NEJM2011)
L’aderenza alla profilassi pre-esposizione
predice in modo impreciso il rischio di
acquisizione dell’infezione
I livelli plasmatici del farmaco predicono in
modo accurato
Risultati paradossali
Lo studio CAST
La fibrillazione ventricolare è ritenuta una delle
principali cause di morte nei pazienti con
infarto
Encainide e flecainide avevano mostrato una
significativa efficacia nel pervenire la
comparsa di fibrillazione in pazienti infartuati
Nel trial clinico i pazienti trattati con questi
antiaritmici avevano una mortalità più alta
Risultati paradossali
Trattamento infezione da MAC in pazienti con AIDS
Dose claritromicina (mg – bid)
Batteriemia
CFU/ml
Mortalità 12
settimane
500
1000
1200
145
34
25
5.7%
25.5%
28%
HIV-RNA e linfociti CD4 come esiti surrogati
negli studi di terapia antiretrovirale
Coll Group AIDS Res Hum Retr 2000
Association Between Sustained Virological Response and AllCause Mortality Among Patients With Chronic Hepatitis C and
Advanced Hepatic Fibrosis
Adriaan J. van der Meer et al. JAMA. 2012;308(24):2584-2593
• An international, multicenter, long-term follow-up study from
5 large tertiary care hospitals in Europe and Canada of 530
patients with chronic HCV infection who started an nterferonbased treatment regimen between 1990 and 2003, following
histological proof of advanced hepatic fibrosis or cirrhosis
(Ishak score 4-6). Complete follow-up ranged between
January 2010 and October 2011.
• Main Outcome Measures All-cause mortality. Secondary
outcomes were liver failure, HCC, and liver-related mortality
or liver transplantation
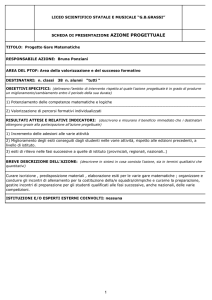
Association Between Sustained Virological Response and AllCause Mortality Among Patients With Chronic Hepatitis C and
Advanced Hepatic Fibrosis
Adriaan J. van der Meer et al. JAMA. 2012;308(24):2584-2593
10-year cumulative incidence rate
of all-cause mortality 8.9% with
SVR and 26.0% without SVR
10-year cumulative
incidence rate of liverrelated mortality or
transplantation 1.9% with
SVR and 27.4% without SVR
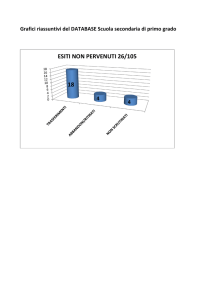
Association Between Sustained Virological Response and AllCause Mortality Among Patients With Chronic Hepatitis C and
Advanced Hepatic Fibrosis
Adriaan J. van der Meer et al. JAMA. 2012;308(24):2584-2593
10-year cumulative incidence rate
of HCC 5.1% with SVR and 21.8%
without SVR
10-year cumulative
incidence rate of liver failure
2.1% with SVR and 29.9%
without SVR
Un valido esito surrogato:
• è un elemento della catena causale che porta
al manifestarsi della malattia e se l’effetto del
farmaco sulla malattia è mediato dal suo
effetto sul marcatore
• le sue variazioni nel tempo si associano con le
variazioni del rischio di eventi clinici
• le variazioni che si osservano in seguito alla
terapia rendono conto completamente (o
quanto meno in grandissima parte) delle
variazioni del rischio di eventi clinici.
Il futuro degli esiti surrogati
http://www.informaazione.info/files/eBooks/Farma_
e_Co.pdf