Il contornamento su immagini PET
di lesioni
in organi in movimento
Roberta Matheoud
SCDO Fisica Sanitaria
AOU Maggiore della Carità, Novara
Torino, 14 dicembre 2012
L’imaging
multimodale
(CT+PET+MR)
nel
trattamento
radioterapico consente di ottenere dati complementari alla
delineazione del tumore.
La
natura
interdisciplinare
di
questo
approccio richiede la collaborazione di diverse
figure professionali (radioterapista, medico
nucleare, fisico, TSRM, …)
Con l’introduzione della IGRT che permette di modificare il
fascio durante il trattamento e da un trattamento all’altro,
l’accuratezza nell’individuazione del bersaglio è d’obbligo.
I TUMORI DEL TORACE E DELL’ADDOME
SI MUOVONO …
… con il movimento respiratorio del paziente, di ~ 2-3 cm nella
direzione cranio-caudale …
Incertezza della posizione del tumore durante il
ciclo respiratorio
in passato trattati volumi maggiori del tessuto
normale
maggiore probabilità di danneggiare
strutture sane in prossimità del tumore.
le
Più critico è il problema del sottodosaggio dei bordi del tumore,
perchè potrebbe muoversi al di fuori dei confini prestabiliti.
L’IGRT consente di sincronizzare
l’emissione della dose terapeutica
di radiazione a seconda della fase
del ciclo respiratorio del paziente:
Ovviamente per poter fare ciò è necessario che anche in
fase di simulazione l’imaging fornisca analoghe informazini
spazio-temporali per ‘colpire’ la lesione in una determinata
fase del respiro.
QUALE TECNICA PER SIMULARE ? …
1. Breath-hold CT
2. Respiratory-gated CT
3. Breath-hold PET or respiratory-gated PET/CT
FACCIAMO UN PASSO
INDIETRO …
… BREVE ACCENNO AL CONTORNAMENTO
SULLE IMMAGINI STATICHE …
A causa della limitata risoluzione spaziale delle immagini PET
(benchè migliore rispetto a quella della MN tradizionale) la
delineazione di una lesione captante FDG ai fini del suo
trattamento in radioterapia con fasci esterni è un problema di
non banale soluzione
Pertanto diverse strategie di contornamento sono
state proposte
E a tutt’oggi il problema non presenta una soluzione
univoca ….
Metodi di contornamento
sulle immagini PET statiche
1. Contornamento ‘manuale-visivo’ effettuato da medici
radioterapisti esperti
2. Soglia assoluta: Standardized Uptake Value (SUV) >2.5
3. Soglia fissa: percentuale fissata della massima
concentrazione di tracciante nella lesione ovvero del
SUV medio
SUV>2.5
40%
4. Algoritmi dipendenti dalla dimensione della lesione Th = f(lesione)
5. Algoritmi dipendenti dal contrasto
6. Algoritmi complessi
Th = f(CNRlesione)
Pro’s e Con’s dei metodi di contornamento
Metodo
1.Manuale
semplice
Operatore dipendente
2.SUV assoluto
semplice
Assunzione: SUVles pat > 2.5
FALSO !!!
3.% fissa <SUV>
semplice Serve ROI per definire <SUV>
ragionamento circolare
4. f=f(dimensione lesione)
?
La dimensione è quella che
vogliamo conoscere
5. f=f(contrasto lesione)
funziona
Sono scanner specifici
6. f=f complessa
funziona
Piattaforma speciale
(fuori da RT planning)
Quindi, eliminati i metodi che si è dimostrato non funzionare:
1. Manuale
2. SUVmax > 2.5
3. Percentuale fissa del SUV medio
Rimangono gli altri, che possiamo raggruppare in:
Algoritmi dipendenti dal contrasto:
f = f(, CNR, recon-param/PET)
Algoritmi complessi:
f = fuzzy, m.gradienti, …
Se poi consideriamo
Un bersaglio in movimento
… ci rendiamo conto che la probabilità di colpirlo dipende da:
Ampiezza del movimento
Velocità del movimento
la delineazione di una lesione in movimento sulle immagini
PET è un problema non banale.
Possiamo pensare di colpirlo in una posizione media delle
posizioni assunte durante il movimento oppure di sparare
sincronizzando la ‘pistola’ con il suo movimento a patto di
conoscerlo.
O usiamo una sua immagine mediata
Oppure un’immagine 4D (info spazio-temporali)
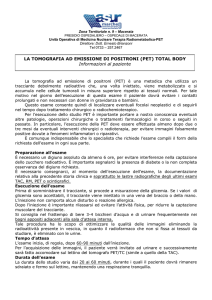
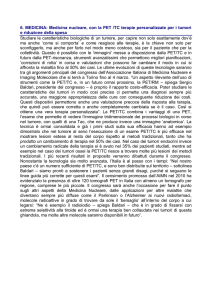
Come si muove una lesione
polmonare ?
Studiate 1295 tracce !!!
The respiratory trace acquired by the RPM system is the
vertical displacement of the marker as a function of time.
This trace is considered to be a surrogate for internal
organ motion.
Classificate in 3 tipi distinti:
Type-1: a prominent peak at the low end
(the patient’s breathing cycle consistently
returns to a similar location at endexpiration and tends to spend more time
near end-expiration).
~60%
Type-2: could be caused by numerous
respiratory patterns including variable endexpiration locations or similar inspiratory
and expiratory phase lengths.
~20%
Type-3: no recognizable shape and is
simply spread out over the histogram bins.
This is usually caused by the long-term
variability of the respiratory trace.
~20%
Liu, PMB2009
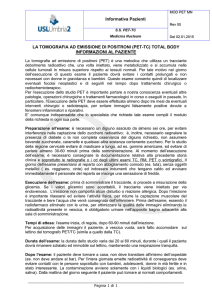
Cosa comporta il movimento
della lesione ?
Liu, PMB2009
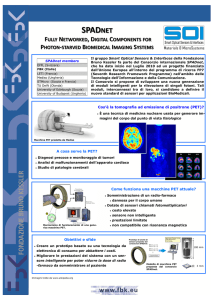
Experimental setup. Data Spectrum® Anthropomorphic cardiac-torso phantom
(heart, lungs, liver and spine inserts).
Two spherical ‘lesions’ into the lung (=1.1cm) and liver (=1.4cm), with lesionto-background ratio of 8:1.
Phantom positioned on the QUASAR® programmable respiratory motion platform
from Modus Medical Devices Inc. (London, Ontario, Canada).
Canonical 8 min, type-1 trace to an 11 mm motion to drive the QUASAR® platform
to translate the phantom during scanning. We measured weight-based SUV.
Liu, PMB2009
Simulation.
NURBS-based cardiac torso phantom with the same FDG organ activity distribution as
that of the phantom experiment.
To simulate whole-body PET acquisition of a free breathing patient, a (4D) NCAT
phantom dataset by generating 200 three-dimensional (3D) NCAT phantoms with
diaphragm displacements equally sampled over a 4 cm amplitude.
Motion-blurred sinograms simulated for all 1295 patient RPM traces with different
amplitudes using the NCAT phantom.
Liu, PMB2009
Results. Mean motion amplitude is 10.9 mm for the left diaphragm and 10.1 mm for
the right diaphragm.
SUVmax for both lesions reduced in the motion-blurred image compared to those in
the no-motion image.
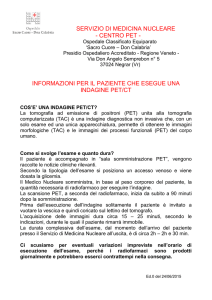
Errore frazionale del SUVmax
Lesions in the lower lung region more blurred than those in the middle and upper
lung regions, and upper lung lesions were the least affected by respiratory motion in
general:
Liu, PMB2009
• Errors >> for lesions in upper lung, middle lung and liver (>> motion amplitudes)
• For lower lung lesion, there is a trend that larger motion amplitudes lead to
smaller errors, mainly as a result of artifacts due to mismatched attenuation
correction at larger motion amplitudes:
Liu, PMB2009
• Larger motion amplitude greater errors of SUVmax and
volume;
• Larger lesions less subject to respiratory motion than smaller
lesions;
• Lesions in the upper lung region smaller errors in SUVmax and
volume.
Conclusions
It can be critical to correct for respiratory motion in clinical practice
to improve quantification and treatment planning in oncological
PET/CT imaging.
Liu, PMB2009
Il movimento influenza il SUV…
Ma il SUV influisce sul contornamento
della lesione …
Come possiamo contornare
lesione in movimento ?
una
Potremmo cercare di fermarla,
congelandola in un istante del
ciclo respiratorio, ma …
Questa tecnica (DEEP INSPIRATION-BREATH HOLD
TECHNIQUE) può non essere realizzabile da parte di
pazienti molto malati, specialmente da parte di quelli
con ca polmonare, cioè quelli di nostro interesse.
Evaluation of the combined effects of target
size, respiratory motion and backgroud activity
on 3D and 4D PET/CT images
SJ Park, PMB 2008
What is the best methodology for applying 4D PET/CT to moving
target definition ?
3 acquisition protocols tested:
1- 3D PET/3D CT: ungated PET + ungated CT
2- 4D PET/4D CT: respiratory-gated PET + 4D attenuation maps
3- 4D PET/3D CT: respiratory gated PET + ungated CT
Park, PMB2008
Phantoms
Dynamic thorax phantom: average human thorax with hollow sphere
phantom filled with FDG inserted in the lung cylinder, TB=infinity
Cranio-caudal motion
Nema IEC body phantom: spheres with TB=8 and 4.
Gating. 4D-PET rebinned into 1.2.5.10 and 20 phases.
Park, PMB2008
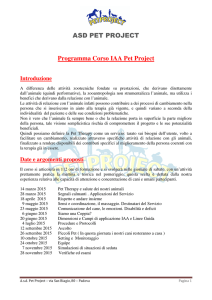
Analisi
Analizzate le seguenti figure di merito:
• Coefficiente di recupero del contrasto, RC = Aobs/Atrue
• Coefficiente di recupero del volume, VRC = Vmeas/Vtrue
• Rapporto segnale-rumore, SNR
• Rapporto contrasto-rumore, CNR
Park, PMB2008
Results
Blurring/Smearing effects induced from respiratory motion:
Activity concentration
0.5 ml sphere
Activity concentration
no motion
Park, PMB2008
16 ml sphere
RC identico
per 4D-PET con fantoccio in movimento
e 3D-PET con fantoccio statico
Park, PMB2008
SNR e CNR
Park, PMB2008
RC with 5 bins were almost equal to the standard reference values.
VRC with < 5bins were overestimated, with >10 bins underestimated
at TB 8 and 4.
Thresholds applied to 4D_PET images of moving targets are
similar to those for 3D_PET of resting targets.
Park, PMB2008
Conclusioni
• 4D-PET recupera con successo ciò che si perde con il
movimento (RC e VRC).
• Il gating a 5-bin fornisce la migliore risoluzione temporale
con un rumore ridotto sull’immagine.
• I risultati basati sul protocollo 4D possono essere utilizzati
per migliorare l’accuratezza nel determinare il GTV dei tumori
polmonari.
Quindi 4D-PET è meglio della 3D-PET … ma …
Park, PMB2008
AIM:
to investigate the correlation among anatomic tumor size on
CT, the 18F-FDG uptake level of heterogeneity, and the
differences between various automatic PET metabolically
active tumor volume (MATV) delineation approaches.
Hatt, JNM 2011
METHODS
25 pts with NSCLC (stage Ib–IIIb)
Free-breathing PET and CT images
Within a week after PET/CT acquisitions, 17 of the 25
patients underwent surgery (measured the maximum
diameter of the tumor).
PET and CT Tumor Delineation:
1. A fixed threshold at T50,
2. an adaptive threshold taking into account the background
uptake (2 obs’),
3. fuzzy locally adaptive Bayesian (FLAB) algorithm
Hatt, JNM 2011
ANALYSIS
• Maximum diameter measured and compared with the
histopathologic reference;
• Anatomic tumor volumes on CT and MATV obtained by
each delineation approach compared;
• 18F-FDG heterogeneity estimated using the coefficient
of variation (CV%)
Hatt, JNM 2011
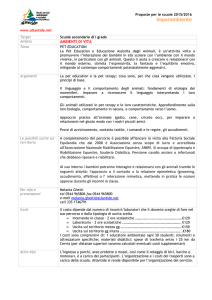
RESULTS
Measured diameters correlated strongly with macroscopic
examination and PET-CT measurements.
Hatt, JNM 2011
La correlazione migliore è tra la
misurazione macroscopica e FLAB:
Hatt, JNM 2011
CONCLUSION
• CT volumes > PET based volumes
• tumor size and PET uptake heterogeneity significant
impact on the MATV PET
• large, heterogeneous NSCLC, largely underestimate MATV
(threshold approache only for small lesions with sufficient TB
ratio or for large/ homogeneous tumors)
• For accurate automatic delineation of MATV in NSCLC,
advanced image segmentation algorithms should be used.
Hatt, JNM 2011
Aim
To compare metabolic tumor volume assessments derived from
SUV and Patlak images using a variety of (semi-)automatic tumor
delineation methods in order to identify methods that can be used
reliably on (whole body) SUV images.
Cheebsumon, EjNMMI 2011
Patlak analysis: accurate method for estimating glucose metabolic
rate, but impractical, as it typically requires a full dynamic study
from injection to about 60 min and limits data acquisition to a single
bed position with an axial coverage of < 20 cm.
METHODS
10 NSCLC (stages IIIB to IV) patients
• Dynamic FDG PET scans
• Blood samples for determining plasma glucose levels were
collected at fixed times (i.e., at 35, 45, 55 min post injection).
• Summed image (45 to 60 min post injection) used to generate a
SUV image.
Cheebsumon, EjNMMI 2011
DATA ANALYSIS
Metabolic tumor volume assessed with:
• Fixed threshold of 50% and 70% (VOI50, VOI70)
• Adaptive threshold of 41%, 50%, and 70% (VOIA41, VOIA50,
VOIA70)
• Contrast-oriented method (VOISchaefer)
• Background-subtracted relative-threshold level [RTL] method
(VOIRTL). (iterative method + PSF convolution)
• Gradient-based watershed segmentation method
Cheebsumon, EjNMMI 2011
Both metabolic volumes and differences in measured volumes
derived from two image types are reported. The percentage volume
difference was defined as (VolumeSUV/VolumePatlak – 1) × 100%:
N° outliers
Cheebsumon, EjNMMI 2011
Volume da SUV
Cheebsumon, EjNMMI 2011
Volume da Patlak
CONCLUSION
• Large differences may exist in metabolic volumes derived
from static (SUV) and dynamic (Patlak) FDG image data.
• These differences depend strongly on the delineation
method used.
• (Semi-)automatic tumor delineation contrast-based
methods provide the most consistent results between
SUV and Patlak images.
Cheebsumon, EjNMMI 2011
RIASSUMENDO …
• Il movimento della lesione ha un effetto importante sul
SUV: la correzione è un aspetto molto critico per migliorare
la quantificazione (Liu, PMB2009)
• 4D PET (5 bin) recupera RC e VRC e quindi migliora
l’accuratezza nella delineazione del GTV (Park, PMB2008)
• CT per delineare non va bene (VCT >> VPET)
Gli algoritmi a soglia non vanno bene per delineare lesioni
eterogenee
L’algoritmo di delineazione migliore è FLAB (algoritmi
complessi, fuzzy) (Hatt, JNM2011)
• I metodi di delineazione a gradiente che correggono per il
rapporto SNR locale (attorno alla lesione) sono i migliori
(immagini 3D PET) (Cheebsumon, EJNMMI 2011)
CONCLUSIONI
… e quindi ?
Il ‘coro’ di voci indica che 4D-PET è meglio di 3D_PET
Un conto è l’acquisizione 4D_PET, un altro è la delineazione del
volume bersaglio, un altro ancora è l’esportazione delle VOI sulla WS
dei piani di trattamento.
L’uso degli algoritmi complessi per la delineazione dei volumi sembra
essere molto promettente, MA …
… questi algoritmi necessitano di software dedicati e costosi (Matlab,
IDL) e di piattaforme diverse dalla WS-PET o WS-RT …
… cioè non sono implementabili con facilità nella pratica clinica …
… e sulla base della mia esperienza personale, ciò che non è
semplice all’uso anche se estremamente accurato, non viene poi
utilizzato.
Al momento, non trascurerei le voci di Hatt e Cheebsumon
che hanno utilizzato con successo una 3D-PET (pur con
gradienti e FLAB)
… e se riprendiamo il grafico:
… ci accorgiamo che anche il metodo a soglia basato sul
contrasto poi non è tanto male … ed è semplice da usare !!!