Cardiogenic Shock (CS) in AMI
Definition
• CS is a state of impaired end-organ perfusion owing to a
reduced cardiac output ( hypotension and impaired
tissue perfusion).
Assistenza Respiratoria Extracorporea:
quando opportuna e quando indispensabile
• Systolic blood pressure (SBP) < 90 mmHg for more than 30’ ( no
hypovolemia) or vasopressor required to achieve a SBP > 90
mmHg
• Cardiac Index (CI) < 1.8 L/min/m2 ( or 2.0-2.2 with support)
• LV filling pressure (WP) > 18 mmHg
• Vital organ hypoperfusion
– cool extremities
– Decrease urine output and/or alteration in mental status
– + serum lactate measurement
FABRIZIO OLIVA
PS: CS diagnosis not necessarily need invasive measurements
CARDIOLUCCA 2013, Il Grand Tour della Cardiologia
Luvva 29 Novembre 2013
IN-HF Outcome
F. Oliva
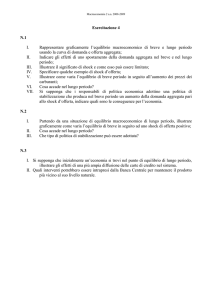
Acute HF: All-cause mortality
by clinical profile at entry
22.6%
22.6%
Cause
(n. 164)
(n. 814)
15.8%
(n. 1855)
(n. 239)
(n. 42)
(n. 501)
(n. 95)
Oliva et al EJHF 2012
F. Oliva
Cardiogenic Shock
Cardiogenic Shock
• Sindrome coronarica acuta
– ampia estensione area ischemica
– in pz con compromissione funzione VS
– complicanze meccaniche (rottura papillare, difetto
IV, rottura parete libera)
– infarto VD
• Scompenso acuto in preesistente cardiomiopatia
ipocinetica end stage
• Miocardite
• Cardiomiopatia ipertrofica ostruttiva
• Patologie valvolari
• Mixoma atriale sinistro
38.1%
23.4%
F. Oliva
Shock Cardiogeno
32.2%
24.0%
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
Cardiogenic Shock (CS) in AMI
Cardiogenic Shock (CS) – TREATMENT
Pathophysiology-Current Concept
Revascularization
1. Hochman JAMA 2001
2. Hochman JAMA 2006
3. Urban Eur Heart J 1999
4. Sanborn JACC 2003
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
Cardiogenic Shock (CS) – TREATMENT
Fluid, Vasopressors, Inotropes
• Initial stabilization with volume expansion to obtain
optimal filling pressures.
• The choice of vasopressor and inotropic therapy is
based on individual experience, institutional policy and
pathophysiological considerations1,2.
• Recent trial: dopamine was associated with more
adverse events3.
Titolo:
Autore:
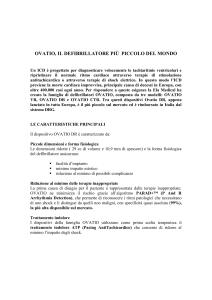
Protocollo Operativo per lo Shock Cardiogeno
In presenza di indicatori clinici e strumentali di
SBP* che permangono dopo cauto test volemico
Data:
Evento:
International Journal of Cardiology 2011, 149: 384
*Raccolta parametri
clinici e lab se pz
esterno
Contattare:
Cardiologo
Rianimatore
Cardiochirurgo
Adeguamento terapeutico
Monitoraggio avanzato
Adrenalina >0,05γ/Kg/min
+ altro inotropo
>6 PVC< 12 mmHg
VAM se indicata
Swan-Ganz - ECO
Rivalutazione dopo 2 h
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
1. Antman Circulation 2004
2. Wan Der Weerf Eur Heart J 2008
3. De Backer N Engl J Med 2010
Cardiogenic Shock
Cardiogenic Shock
Mechanical Support: When?
Protocollo Operativo per lo Shock Cardiogeno
Rivalutazione dopo 2 h
Non miglioramento
(Lattati/SVO2/QU)
Miglioramento
(Lattati/SVO2/QU)
IABP
Continua terapia
medica
Rivalutazione
dopo 1 h
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock (CS) – TREATMENT
IABP
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
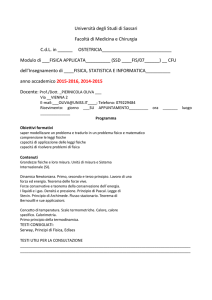
2006: IABP Use
in ESC and Italian Registries
Cardiogenic Shock (CS) – TREATMENT
IABP
• The effects on cardiac output are only modest.
• It’s the more widely used mechanical support device for
CS.
• It’s reccomended ( class II A AHA/ACC, class II B ESC).
Percentage of IABP used in selected trials and registries
2,5
35,0
30,0
2,0
25,0
1,5
20,0
Eur 2006
• Few randomized clinical trials.
• Registries: conflicting results in mortality risk differences
Ita 2006
1,0
Ita 2006
10,0
– Pre-fibrinolytic era 28% favour IABP
– Fibrinolytic era
18% favour IABP
– PCI era
6% increase mortality for IABP
0,5
5,0
0,0
0,0
IABP (%Shock)
IABP
Tavazzi et al, Eur Heart J 2006
Nieminen et al, Eur Heart J 2006
Thiele Eur Heart J 2010
F. Oliva
Eur 2006
15,0
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiovascular Outcomes Using Intra-Aortic Ballon
Pump in High-Risk Acute Myocardial Infarction With or
Without Cardiogenic Shock:
A Meta-Analysis
BUT…
Journal of Cardiovascular Pharmacology and Therapeutics 2011, Feb. 18
• Scenario: CS complicating AMI, early revascularization
planned.
• Slightly lower mortality compared other trials and
registries.
• High rate of catecholamine use (90%) may offset the
potential benefit of IABP.
• Exclusion criterion of onset shock > 12 h selected for a
disease more amenable to revascularization.
• Benefit in severe CS is still unsettled.
• No information about long-term outcomes.
A systematic review of literature identified 16 studies
In patients with AMI with cardiogenic shock (SBP < 90 mmHg), there was significant reduction in
mortality using IABP. The use of IABP is associated with increase in the rate of both moderate
and severe bleeding.
Cardiogenic Shock
F. Oliva
Thiele N Engl J Med 2012
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
Cardiogenic Shock (CS) – TREATMENT
Percutaneous LV Assist Devices
• When ?
IABP
Rivalutazione
dopo 1 h
Classe IIb
Non miglioramento
(Lattati/SVO2/QU)
( “may be considered”)
In many patients with severe depression of LV
function, haemodynamic support and LV unloading
Idoneità a assistenza
al circolo?
derived
from IABP is insufficient
to reverse CS.
SEVERE
REFRATORY
CARDIOGENIC
SHOCK
(SRCS)
The use of percutaneous
LV assist devices with active
Classe IIa
( “can be useful”)
Miglioramento
(Lattati/SVO2/QU)
NO
SI
circulatory support might be beneficial in CS patients
not responding to standard treatment including IABP
support.
Continua
terapia medica
+ IABP
ECMO/VAD
MCS – ANMCO 2013
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
• NO “assistenza meccanica al circolo di lungo termine”
Goals for a Temporary Support System
• Improve end-organ perfusion
– Blood pressure
– Cardiac output
• Decrease pulmonary capillary wedge
pressure
• Decrease myocardial oxygen consumption
J Heart Lung Transplant 2012;31:117–26
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
:
:
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
?
J Heart Lung Transplant 2010;29:1-10
?
30
2012
2012
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
Extracorporeal Membrane Oxygenation
(ECMO)
ECMO
Effetti dell’ECMO
Circuito preassemblato:
Limiti dell’ECMO
- Aumenta il flusso coronarico.
preserva la vitalità miocardica
favorisce recupero circolazione
spontanea
- Calibro delle cannule.
complicanze vascolari
- Fornisce sangue ossigenato a
cervello, reni ed agli altri
organi.
previene la disfunzione
multiorgano
- Incremento del postcarico
eccessiva introduzione in aorta
ascendente
- No “unloading” del ventricolo sn.
- Pompa centrifuga a flusso continuo
- Ossigenatore
- Scambiatore di calore
- Cannula arteriosa di 17-19 F
- Stabilizza il paziente.
diagnosi eziologica
trattamento
- Cannula venosa di 21-25 F
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
- Durata di supporto limitata.
giorni/settimane
- Necessità di un perfusionista.
Lancet 2008; 372: 512.
Cardiogenic Shock
Indicazioni ECMO
Indicazioni ECMO in UTIC
Indicazioni post-cardiotomiche:
• “Bridge to recovery” nell’insufficienza cardiaca
acuta;
• Incapacità di svezzamento dal BPCP (CEC);
• Disfunzione ventricolare sinistra progressiva
• Ipertensione polmonare
• “Graft failure”
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
• Cardiomiopatia end-stage in terapia medica massimale, in attesa
di trapianto cardiaco o VAD
• Infarto miocardico acuto complicato da shock cardiogeno
refrattario
• Miocardite acuta con severa insufficienza d’organo o aritmie
ventricolari subentranti non controllabili con terapia medica e IABP;
• Embolia polmonare massiva con grave compromissione della
funzionalità ventricolare destra e shock cardiogeno o ACR
• Grave depressione della funzione cardiaca da intossicazione di
farmaci o sepsi
• Arresto cardiaco nel paziente giovane adulto con precoce
rianimazione cardiopolmonare (con verosimile ottima prognosi
neurologica) refrattario a terapia rianimatoria medica ed elettrica. La
durata del supporto con ECMO dovrà essere il più breve possibile
(sconsigliato per più di 3 giorni). [Da associare ad altre strategie di
neuroprotezione come l’ipotermia terapeutica]
F. Oliva
Cardiogenic Shock
Indicazioni ECMO in UTIC
…..no study has provided clear evidence of
the merits of extracorporeal life-support in patients
with out-of-hospital cardiac arrest.
Cardiotoxicity, severe accidental
hypothermia, and recurrent ventricular fibrillation
are three widely accepted indications for emergency
cardio pulmonary bypass support in patients
with protracted cardiopulmonary arrest
outside the catheter
laboratory….
Lancet 2008, Editorial
F. Oliva
Cardiogenic Shock
“Bridge to Bridge”
F. Oliva
Cardiogenic Shock
• L’indicazione all’ECMO, nel caso di grave scompenso cardiaco
non più responsivo a terapia medica massimale, dovrà tenere conto
– della prognosi, in particolare ripresa della funzionalità dell’organo
[bridge-to-recovery],
– dell’eleggibilità per un trapianto cardiaco [bridge-totransplantation],
– della possibilità di posizionamento di assistenze meccaniche più
o meno a lunga durata (come Levitronix CentriMag, Jarvik
2000, Cardiowest) [bridge-to-bridge].
– Ma anche ……….. bridge to decision.
F. Oliva
Cardiogenic Shock
“Bridge to Transplant”
•Temporary support
•Long standing HF, Severa AMI,
Giant cells myocarditis
•Not expected to recovery
If recovery does not
occur, it’s possible to
switch toward a Long
Term Device
Persistent low blood pressure (systolic blood pressure < 80 mm Hg for adults) and oliguria
(< 0.5 mL/kg/hr) for at least 4 hours despite maximal inotropic support and IABP
To allow the patient to wait for
early heart transplant
“Bridge to Recovery”
•AMI, Fulminant myocarditis, postpartum cardiomyopathy, postcardiotomy shock
To allow the heart to rest,
expecting short-term recover
• Implanted peripherally in 8 cases (53.4%) and centrally in the remaining 7 (46.6%).
• Mean veno-arterial extracorporeal membrane oxygenation duration was 11.5 ± 8.1
days (range, 1–30)
J Thorac Cardiovasc Surg 2010;140:1416-21
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
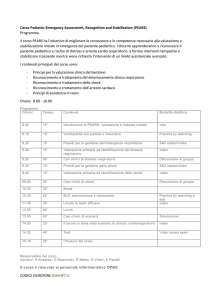
ECMO: LA RETE
I Percorsi Assistenziali
HUB di riferimento
I Level:
II Level:
UTIC
IABP
Necessità
Necessità di:
Numero telefonico dedicato
Equipe impianto ECMO H 24
Disponibilità
Disponibilità posto letto dedicato
• In relazione al contesto locale:
– Adattare le raccomandazioni delle LG
– Definire:
UTIC
IABP
Cath Lab
+ Surg
ECMO
•
•
•
•
Procedure (how)
Professionisti (who)
Setting (where)
Tempistiche (when)
Priorità
Priorità:
Equipe ECMO in centro SPOKE
Valutazione se impianto ECMO in
centro SPOKE e in quale sede
(UTIC/emodinamica/sala operatoria)
Stabilizzazione e trasporto protetto
(con o senza ECMO) del paziente
III Level: Transplant or VAD Center
UTIC SPOKE
Necessità
Necessità di:
valutazione indicazioni
stabilizzazione e preparazione del
paziente in accordo con centro HUB
Priorità
Priorità:
Contattare HUB di riferimento
Concordare modalità
modalità di stabilizzazione
con protocolli condivisi
Stabilire sede di impianto
programmare e concordare trasporto
ECMO VAD TC
F. Oliva
Cardiogenic Shock
Cardiogenic Shock
INFERENCES
• CS is a dramatic medical condition that requires a quick
and multidisciplinary approach.
• All Cardiological Intensive Care Units should be able to
implant a IABP when the drugs failed.
• In severe refractory cardiogenic shock emergency
transfer to an experienced center ( Mobile Cardiac
Assistance Unit)
–
–
–
–
F. Oliva
ECMO first line therapy , insitution before MOF
ECMO as a bridge to… whatever seems reasonable
20-40% of long-term survivors (poor oucomes if MOF)
Bigger devices ? Second line strategy if long term strategy is
required
Cardiogenic Shock
F. Oliva
Cardiogenic Shock
F. Oliva
Mezzo di trasporto dedicato H 24
Cardiogenic Shock