Guida alla terapia
dell’Ipertensione
Arteriosa Polmonare
Carlo D’Agostino
Cardiologia Ospedaliera
Policlinico Bari
C
a
DISCLOSURE INFORMATION
• Carlo D’Agostino
negli ultimi due anni non ho avuto rapporti anche di
finanziamento con soggetti portatori di interessi
commerciali in campo sanitario
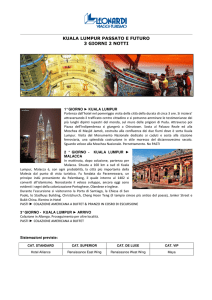
5th World Symposium on PH: Modified classification of PH
1. Pulmonary arterial hypertension
1.1 Idiopathic PAH
1.2 Heritable PAH
1.2.1 BMPR2
1.2.2 ALK1, ENG, SMAD9, CAV1, KCNK3
1.2.3 Unknown
1.3 Drug- and toxin-induced
1.4 Associated with
1.4.1 Connective tissue diseases
1.4.2 HIV infection
1.4.3 Portal hypertension
1.4.4 Congenital heart disease
1.4.5 Schistosomiasis
1’ Pulmonary veno-occlusive disease and/or
pulmonary capillary haemangiomatosis
1’’ Persistent PH of the newborn (PPHN)
5%
3. PH due to lung diseases and/or hypoxia
3.1 COPD
3.2 Interstitial lung disease
3.3 Other pulmonary diseases with mixed
restrictive and obstructive pattern
3.4 Sleep-disordered breathing
3.5 Alveolar hypoventilation disorders
3.6 Chronic exposure to high altitude
3.7 Developmental lung diseases
10%
4. CTEPH
1,5%
5. PH with unclear multifactorial mechanisms
5.1 Haematological disorders: chronic haemolytic
anaemia, myeloproliferative disorders,
splenectomy
5.2 Systemic disorders: sarcoidosis, pulmonary
histiocytosis, lymphangioleiomyomatosis
5.3 Metabolic disorders: glycogen storage disease,
Gaucher disease, thyroid disorders
5.4 Others: tumoural obstruction, fibrosing
mediastinitis, chronic renal failure, segmental
PH
5%
2. PH due to LHD
2.1 LV systolic dysfunction
2.2 LV diastolic dysfunction
2.3 Valvular disease
2.4 Congenital/acquired left heart
inflow/outflow obstruction
78%
Simonneau G, et al. J Am Coll Cardiol 2013; 62:D34-41.
Ipertensione Arteriosa Polmonare - Gruppo 1 OMS
1.
2.
Idiopatica
Ereditaria
1. BMPR2
2. ALK1
3. SCONOSCIUTA
3. Da farmaci e tossine
4. Associata con (APAH)
1. Connettivopatia
2. HIV
3. Ipertensione portale
4. Cardiopatia congenita
5. Schistosomiasi
1.1 IAP veno occlusiva e capillari
1.2 IAP persistente del neonato
Circa il 5% delle PH
Prevalenza = 5,9-15 casi/milione
Incidenza = 2,4 casi/milione/anno
• 39,2% IPAH
• 3,9% FPAH
• 15,3% Connettivopatia
(prevalentemente
sclerodermia)
• 11,3% Cardiopatia congenita
• 10,4% Ipertensione Portale
• 9,5% Anoressizzanti
• 6,2% HIV
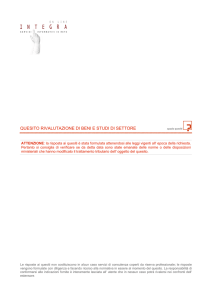
Prognosi dei pazienti con Ipertensione Arteriosa
Polmonare
Classe NYHA alla presentazione
Humbert M, et al . Circulation 2010;122:158-63
Distanza percorsa al 6MWT
alla presentazione
Strategia
Il ricorso motivato e ragionato a mezzi idonei al
raggiungimento di uno scopo.
Devoto-Oli Vocabolario della lingua italiana
La descrizione di un piano d'azione di lungo termine
usato per impostare e successivamente coordinare le
azioni tese a raggiungere uno scopo predeterminato.
Wikipedia
#1 Counselling
#2 Terapia di supporto
#3 Vasoreattività? > Ca antagonisti
#4 Inizio terapia specifica
#5 Rivalutazione periodica frequente
#6 Implementazione/modifica della terapia
(rivalutazione e cateterismo cardiaco)
#7 Terapia interventistica (settostomia/Trapianto….)
Exercise training improves peak oxygen consumption and haemodynamics in patients with severe
pulmonary arterial hypertension and inoperable chronic thrombo-embolic pulmonary hypertension: a
prospective, randomized, controlled trial
Ehlken E et al. Eur Heart J. 2016 Jan 1;37(1):35-44.
Exercise training improves peak oxygen consumption and haemodynamics in patients with severe
pulmonary arterial hypertension and inoperable chronic thrombo-embolic pulmonary hypertension: a
prospective, randomized, controlled trial
Ehlken E et al. Eur Heart J. 2016 Jan 1;37(1):35-44.
Exercise training improves peak oxygen consumption and haemodynamics in patients with severe
pulmonary arterial hypertension and inoperable chronic thrombo-embolic pulmonary hypertension: a
prospective, randomized, controlled trial
Ehlken E et al. Eur Heart J. 2016 Jan 1;37(1):35-44.
Exercise training improves peak oxygen consumption and haemodynamics in patients with severe
pulmonary arterial hypertension and inoperable chronic thrombo-embolic pulmonary hypertension: a
prospective, randomized, controlled trial
Ehlken E et al. Eur Heart J. 2016 Jan 1;37(1):35-44.
#1 Counselling
#2 Terapia di supporto
#3 Vasoreattività? > Ca antagonisti
#4 Inizio terapia specifica
#5 Rivalutazione periodica frequente
#6 Implementazione/modifica della terapia
(rivalutazione e cateterismo cardiaco)
#7 Terapia interventistica (settostomia/Trapianto….)
#1 Counselling
#2 Terapia di supporto
#3 Vasoreattività? > Ca antagonisti
#4 Inizio terapia specifica
#5 Rivalutazione periodica frequente
#6 Implementazione/modifica della terapia
(rivalutazione e cateterismo cardiaco)
#7 Terapia interventistica (settostomia/Trapianto….)
TEST DI VASOREATTIVITA’
Risposta positiva = Riduzione PAPm
≥10 mmHg per raggiungere un valora
assoluto di PAPm ≤40 mmHg con CO
incrementata o immodificata.
#1 Counselling
#2 Terapia di supporto
#3 Vasoreattività? > Ca antagonisti
#4 Inizio terapia specifica
#5 Rivalutazione periodica frequente
#6 Implementazione/modifica della terapia
(rivalutazione e cateterismo cardiaco)
#7 Terapia interventistica (settostomia/Trapianto….)
Humbert M, Sitbon O, Simonneau G: NEJM 2004;351:1425
Meccanismi coinvolti
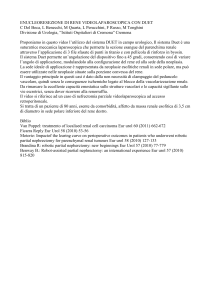
Farmaci approvati per il trattamento della IAP
Approval of PAH therapies
Iloprost inhaled
2004 – US
2003 – Europe
Beraprost†
1999
Bosentan
2001 – US
2002 – Europe
1995
Epoprostenol i.v.
1995 – US
2001 – Europe
Iloprost i.v.
Only approved in
New Zealand
2000
Treprostinil i.v. or s.c.
2002 – US
2005 – Europe
Room-temperature stable epoprostenol i.v.
2012 – US, Switzerland & Canada
2013 – Japan & Europe*
Sildenafil
2005
Beraprost‡†
2007
2005
2010
Ambrisentan
2007 – US
2008 – Europe
*End of decentralised procedure in EU; local approvals ongoing
†Approval of these therapies varies by country, and thus they
might not be approved in the indications mentioned in your
country. Please refer to your local full SmPC before prescribing.
‡Prolonged release derivative
21; 29 March 2015
2009
Treprostinil inhaled†
Tadalafil
2008 – Europe
2009 – US
2015
2013
Macitentan†
Treprostinil oral†
US
Riociguat†
2013 – US
2014 – Europe
Sebbene ci sia stato un miglioramento dell’outcome negli ultimi 15
anni, la prognosi a lungo termine rimane insiddisfacente
Benza RL et al Chest 2012; 142:448-56
Significato prognostico della variazione al follow up
WHO I I
WHO III-IV I-II
WHO I-II III-IV
WHO III-IV III-IV
SvO2 ≥ 65% =
SvO2 <65% ≥ 65%
SvO2 ≥ 65% <65%
SvO2 <65% =
Nickel N, et al . Eur Respir J 2012;39:589-596
CI ≥2,5 L/min/m2
CI <2,5 L/min/m2
CI ≥2,5 L/min/m2
CI <2,5 L/min/m2
=
≥2,5
<2,5
=
NT-proBNP <1800 =
NT-proBNP ≥1800<1800
NT-proBNP <1800 >1800
NT-proBNP ≥1800≥1800
Scelta della strategia terapeutica
• Monoterapia iniziale
– Con quale farmaco?
– Come proseguire?
• Terapia di combinazione iniziale
– Con quali farmaci
– Come proseguire?
Possibili terapie di associazione
Antagonisti Recettoriali
della ET-1
Prostanoidi
(e.v., s.c., os, inal)
Inibitori della
Fosfodiesterasi 5
o GCS
All-cause death
OR
Atrial septostomy
Time to 1st
morbidity or
mortality event
OR
Lung
transplantation
OR
Initiation of i.v. or
s.c. prostanoids
OR
Other worsening
of PAH OR
A decrease in 6MWD of at least 15%,
confirmed by 2 tests on different days
AND
Worsening of PAH symptoms, which must
include either:
• An increase in FC, or
• Appearance or worsening of symptoms of
right heart failure
AND
Need for new PAH treatment(s):
• Oral or inhaled prostanoids
• Oral PDE-5 inhibitors
• ERA after discontinuation of study drug
• Intravenous diuretics
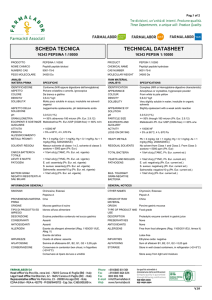
SERAPHIN primary endpoint: Morbidity/mortality
(composite endpoint) up to end of treatment
Patients without an event (%)
Macitentan reduced the risk of a morbidity/mortality event
(composite endpoint) by 45% (hazard ratio 0.55; p < 0.001)
100
80
60
40
20
Macitentan 10 mg
Placebo
0
32; 29 March 2015
0
6
12
18
24
30
36
Patients at risk Time from treatment start (months)
242
208
187
171
155
91
41 Macitentan 10 mg
250
188
160
135
122
64
23 Placebo
Pulido T, et al. N Engl J Med 2013; 369:809-18.
33
Raccomandazioni per la monoterapia nella IAP
Galiè N. et al Eur Heart J 2015, Eur Respir J, 2015
2015; 379(9):834–44.
AMBITION
Combination vs pooled monotherapy
Galie N et al, et al. New Engl J Med 2015; 379(9):834–844.
BONSAI: Six-month results: % change comparison
Mono
(11)
Upfront
Combo (19)
p
RAP (%)
+11 ± 67
-17 ± 50
0.205
mPAP (%)
-19 ± 16
-33 ± 13
0.017
CI (%)
+23 ± 19
+56 ± 31
0.003
PVR (%)
-40 ± 10
-61 ± 12
< 0.001
PA-SO2 (%)
+6 ± 9
+17 ± 11
0.007
6MWD (%)
+10 ± 21
+25 ± 16
0.038
Bachetti C. et al. J Respir Crit Care Med 2015.
4/6-month results: % change comparison
AMBITION - BONSAI
Ambrisentan + Tadalafil
(19)
Joint - INTENTION
Bosentan + Sildenafil
(23)
RAP (%)
-17
- 36
mPAP (%)
-33
- 21
CI (%)
+56
+63
PVR (%)
-61
-60
PA-SO2 (%)
+17
+25
6MWD (%)
+25
+ 42
M. Palazzini et al, ATS 2016.
38
Raccomandazioni per la terapia di combinazione
iniziale nella IAP
Galiè N. et al Eur Heart J 2015, Eur Respir J, 2015
#1 Counselling
#2 Terapia di supporto
#3 Vasoreattività? > Ca antagonisti
#4 Inizio terapia specifica
#5 Rivalutazione periodica frequente
#6 Implementazione/modifica della terapia
(rivalutazione e cateterismo cardiaco)
#7 Terapia interventistica (settostomia/Trapianto….)
#1 Counselling
#2 Terapia di supporto
#3 Vasoreattività? > Ca antagonisti
#4 Inizio terapia specifica
#5 Rivalutazione periodica frequente
#6 Implementazione/modifica della terapia
(rivalutazione e cateterismo cardiaco)
#7 Terapia interventistica (settostomia/Trapianto….)
Raccomandazioni per la terapia sequenziale nella
IAP
Galiè N. et al Eur Heart J 2015, Eur Respir J, 2015
43
#1 Counselling
#2 Terapia di supporto
#3 Vasoreattività? > Ca antagonisti
#4 Inizio terapia specifica
#5 Rivalutazione periodica frequente
#6 Implementazione/modifica della terapia
(rivalutazione e cateterismo cardiaco)
#7 Terapia interventistica (settostomia/Trapianto….)
5th World Symposium on PH: Evidence-based treatment
algorithm
Combination therapy and interventional procedures
Initial therapy with PAH approved drugs
Inadequate clinical response
Sequential combination
therapy (I-A)
ERAs
Prostanoids
+
+
+
Inadequate clinical
response on
maximal therapy
PDE-5i
or sGCS
BAS (IIa-C)
Galiè N, et al. J Am Coll Cardiol 2013; 62:D60-72.
Consider eligibility for
lung transplantation
Referral for
LUNG TRANSPLANTATION
(I-C)
46
Recommendations for evaluation of severity of pulmonary
arterial hypertension and clinical response to therapy
Galiè N. et al Eur Heart J 2015, Eur Respir J, 2015
Definizione della prognosi nella IAP
2015 ESC/ERS Guidelines
REAL IP
REGISTRO ITALIANO IPERTENSIONE POLMONARE