Review
SARS-Coronavirus, an emerging pathogen:
what are the implications for the safety of blood transfusion?
Giancarlo Icardi(1), Filippo Ansaldi(2), Roberto Gasparini(3)
(1)
(2)
(3)
Department of Health Sciences, University of Genoa; Standing Group for the control of SARS - Ministry
of Health, subgroup on epidemiological scenarios
Department of Public Health, University of Trieste; Standing Group for the control of SARS - Ministry
of Health, subgroup on diagnosis and subgroup on SARS and blood donation
Department of Health Sciences, University of Genoa; Standing Group for the control of SARS - Ministry
of Health, subgroup on epidemiological surveillance
Emerging pathogens: from appearance
to epidemic risk
I patogeni emergenti: dalla comparsa
al rischio epidemico
In the last twenty-five years the epidemiological picture
of transmissible diseases has been characterised by the
appearance and identification of an ever increasing number
of micro-organisms. In particular, new viruses have
appeared in the human clade and have been recognised as
the cause of new diseases: the long list includes whole
families such as the Retroviridae whose members Human
T-cell Lymphotropic Virus type-1 (HTLV-I) and Human
Immunodeficiency Virus (HIV) were discovered in 1980
and 1983, or viruses affecting the same target organ, such
as the major hepatotrophic viruses, including hepatitis C
virus, delta viroid and hepatitis E virus, identified at the
end of the 1980s and in the early years of the 1990s1.
Other viruses, such as the West Nile Virus and the
Monkeypox Virus, micro-organisms discovered decades
ago, have recently reappeared in epidemic form, raising
concern and alarm because of their rapid spread in
developed countries2-5.
The reasons for the increase in the so-called emerging
viruses are numerous and complex: the introduction and
spread of molecular techniques capable of identifying and
characterising the genome of micro-organisms with a high
degree of sensitivity and specificity have undoubtedly
played an important role, but it is equally clear that social,
ecological and epidemiological changes have led to
increased contact between men and animals and to faster
circulation of the micro-organisms. The demographic
Da cinque lustri il quadro epidemiologico delle malattie
trasmissibili è stato caratterizzato dall'introduzione e
dall'identificazione di un numero sempre maggiore di
microrganismi. In particolare, nuovi virus si sono affacciati
nel clade umano e sono stati riconosciuti causa di nuove
malattie: il lungo elenco comprende intere famiglie come
quella delle Retroviridae a cui appartengono l'Human Tcell Lymphotropic Virus type-1 (HTLV-I) e l'Human
Immunodeficiency Virus (HIV), scoperti nel 1980 e 1983, o
virus caratterizzati dallo stesso organo bersaglio quali gli
epatotropi maggiori, che comprendono il virus dell'epatite
C, il viroide delta, il virus dell'epatite E individuati a cavallo
degli anni ottanta e novanta1. Negli ultimi mesi, altri virus,
quali il West Nile Virus ed il Monkeypox Virus,
microrganismi noti da decenni, sono ricomparsi in forma
epidemica destando allarme e preoccupazione per la loro
rapida diffusione in realtà socio-sanitarie sviluppate2-5.
Le ragioni dell'aumento dei cosiddetti virus emergenti
sono numerose e complesse: un ruolo di grande importanza
è stato sicuramente giocato dall'introduzione e dalla
diffusione di tecniche molecolari in grado di identificare e
caratterizzare con elevata sensibilità e specificità il genoma
dei microrganismi, ma è fuori di dubbio che i mutamenti
sociali, ecologici ed epidemiologici hanno determinato, da
un lato, un aumento dei contatti tra uomo e animale e,
dall'altro, una più rapida circolazione dei microrganismi.
L'esplosione demografica ha determinato aree del nostro
pianeta caratterizzate da una considerevole biodiversità e
da un'elevata densità abitativa, condizione in cui i contatti
tra uomo e animale e la trasmissione di microrganismi da un
clade all'altro possono essere più frequenti. Una regione
in cui questo fenomeno è particolarmente evidente è
Correspondence:
Prof. Giancarlo Icardi
Dipartimento di Scienze della Salute
Via Pastore 1
16132 Genova
Blood Transf 2003; 3: 215-23
215
G Icardi et al.
explosion has created areas of our planet with considerable
biodiversity and a high population density, conditions
facilitating contact between man and animals and the
transmission of micro-organisms from one clade to another.
One region in which this phenomenon is particularly evident
is South-East Asia. An outstanding example of the possible
interspecies movement of viruses in this area is the influenza
virus. It seems certain that influenza viruses circulating
among aquatic birds, the natural reservoir of the microorganism, have infected chicken, turkey, swine6, whales7
and have been responsible for epidemics among horses8.
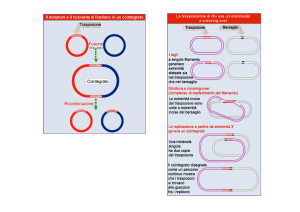
Of more interest, as far as concerns possible consequences
for humans, is the transmission of avian viruses to pigs,
which could represent the mixing vessel between viruses
of avian origin and human viruses. In fact, pigs have some
particular features that make recombination of viral RNA
segments possible during co-infection with both avian and
human viruses, thus allowing the creation of new viruses9,10.
The influenza virus needs a glycoprotein receptor on the
target cell for the replication. This glucidic part of this
receptor terminates with a Sia2-3Gal bond for viruses of
the avian clade and a Sia2-6Gal bond for those of the human
clade. The target cells in pigs have both receptors, making
co-infection possible and also bringing the avian and
human viruses into very close proximity. In these
conditions, the characteristic organisation of the segmented
genome of the influenza virus allows a single gene of the
avian virus to be incorporated into the genome of the human
virus, thus causing recombination of the genetic material
of the micro-organism. This rearrangement between viruses
infecting different species seems to be responsible for the
major variations in the virus, named antigenic shift, and
seems to be implicated in the origin of the influenza
pandemics of the 20th century. The 1957 pandemic, the socalled "Asian flu", originated from the recombination of a
circulating avian H2N2 virus and a human H1N1 virus in
pigs; the resulting pandemic virus had 3 genes of avian
origin (HA, NA, PB1) and the remaining 5 of human origin.
This recombination, having involved the genes coding for
haemagglutinin and neuraminidase, the most important
antigenic determinants, created a virus to which the whole
population was susceptible and thus the conditions
necessary for perpetuation of the pandemic. The
mechanism underlying the appearance of the influenza virus
responsible for the 1968 pandemic, the so-called "Hong
Kong flu" was identical. Avian viruses were reported to
have infected humans directly in southern China in the
second half of the 1990s; in particular, in 1997 and 1999
there were cases of infection with H5N1 and H9N2,
respectively; the jump of the H5N1 virus from chickens,
216
rappresentata dal Sud-Est Asiatico. Un esempio eclatante
del possibile salto interspecie di un virus in quest'area è
espresso dall'influenza. Sembra, infatti, accertato che virus
influenzali circolanti negli uccelli acquatici, reservoir
naturale del microrganismo, abbiano infettato polli, tacchini,
suini6, balene7 e siano stati responsabili di epidemie negli
equini8. Di maggiore interesse, per quanto riguarda i possibili
effetti sull'uomo, è la trasmissione di virus aviari al maiale
che può rappresentare il mixing vessel tra virus di origine
aviaria e virus umani. Il maiale presenta, infatti, alcune
peculiarità che rendono possibile il riassortimento di
segmenti di RNA virale durante la coinfezione di virus aviari
e umani, permettendo la creazione di nuovi virus9,10. Il virus
influenzale necessita, a livello della cellula bersaglio, di un
recettore costituito da una glicoproteina, la cui parte
glucidica termina con un legame Sia2-3Gal per i virus del
clade aviario e Sia2-6Gal per i virus del clade umano. Le
cellule target dei suini presentano entrambi i recettori e
rendono così possibile la coinfezione e la stretta "vicinanza"
di virus aviari e umani. In queste condizioni, la caratteristica
organizzazione del genoma segmentato del virus influenzale
permette che un singolo gene del virus aviario possa essere
incorporato nel genoma di un virus umano, determinando
la ricombinazione del materiale genetico del microrganismo.
Questo meccanismo di riassortimento del materiale genetico
fra virus infettanti specie differenti sembra responsabile
delle cosiddette variazioni maggiori o antigenic shift e
sembra coinvolto nell'origine delle pandemie influenzali che
si sono verificate nel XX secolo. La pandemia del 1957, la
cosiddetta "asiatica", è stata originata dalla ricombinazione
nel suino di un virus aviario circolante H2N2 ed un virus
umano H1N1; il virus pandemico risultante possedeva un
corredo genetico caratterizzato da 3 geni di origine aviaria
(HA, NA, PB1) ed i restanti 5 umani. Il riassortimento,
avendo coinvolto i geni codificanti l'emoagglutinina e la
neuraminidasi, i determinanti antigenici di maggior rilievo,
ha determinato la comparsa di un virus verso cui l'intera
popolazione era suscettibile e ha creato, quindi, quelle
condizioni necessarie per il perpetrarsi della pandemia. Del
tutto analogo il meccanismo che ha determinato la comparsa
del virus influenzale responsabile della pandemia del 1968,
la cosiddetta "Honk Kong". Il salto interspecie diretto di
virus aviari nel clade umano è stato segnalato sempre
nell'area meridionale della Cina nella seconda metà degli
anni novanta; in particolare nel 1997 e 1999, si sono verificati,
rispettivamente, casi di infezione da H5N1 e H9N2; di rilievo
è stato il salto del virus H5N1 dal pollo, dove circolava in
forma epidemica, all'uomo con 18 malati fra gli addetti al
mercato di Honk Kong ed una letalità del 33%11,12.
La comparsa di nuovi patogeni, caratterizzati da una
Blood Transf 2003; 3: 215-23
SARS and blood transfusion
among which it circulated in endemic form, to humans,
infecting 18 market workers in Hong Kong, with a mortality
rate of 33%, was noteworthy11,12.
The appearance of new pathogens with a viraemic
phase, which are potentially transmissible parenterally, is a
problem for transfusion medicine. The rest of this review is
dedicated to the description of a new virus responsible for
an epidemic of atypical pneumonia which has involved
numerous countries in Asia, America and Europe. The main
structural features of the virus are analysed and the current
diagnostic instruments indicated. Finally, the possible risk
of transfusion-related transmission of the new microorganism is considered.
st
The first epidemic of the 21 century
Although the first official notification of an epidemic of
atypical pneumonia was made on February 11th, 2003, the
first cases of Severe Acute Respiratory Syndrome (SARS)
can be traced back to mid-November 2002 in the province
of Guangdong in South China. In the period between the
index case and notification to the World Health Organisation
(WHO), 305 people had fallen ill and 5 had died of the
syndrome. About 30% of the people infected were health
care workers who had come into close contact with the sick
patients. On February 21st, a Chinese doctor who worked in
an out-patients department in the region of Guangdong
moved to Hong Kong and rented a room on the ninth floor
of a hotel in the centre of the city. Over the next few days at
least 12 of the hotel's guests developed early symptoms of
SARS: some of these people were admitted to the Queen
Mary Hospital and to the Prince of Wales Hospital in Hong
Kong, while others continued their journeys and were
admitted to hospitals in Hanoi (Vietnam), Toronto (Canada)
and Singapore13,14. The number of cases multiplied rapidly,
particularly among health care workers in close contact with
patients, and the syndrome spread, carried by international
travellers. New cases of infection were reported in Hong
Kong, Singapore, Canada and China. On March 12th, the
WHO issued a Global Alert and on March 15th, the
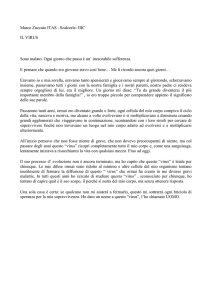
Emergency Travel Advisory. The cumulative number of
cases reported exceeded 5,000 on April 28th, 6,000 on May
2nd and 7,000 on May 8th; 30 countries in 6 continents were
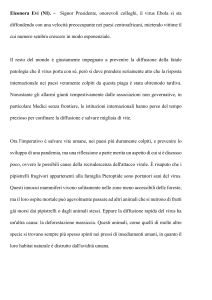
involved by the epidemic. The peak of the epidemic was
reached in the first week of May (Figure 1), during which
1,400 cases were reported. In the following weeks the number
of cases decreased rapidly although there were some alarming
new outbreaks in continental China, Taiwan and Canada
after the epidemic had apparently been controlled. In the
Blood Transf 2003; 3: 215-23
fase viremica e potenzialmente in grado di trasmissione
parenterale, rappresenta una potenziale problematica di
medicina trasfusionale. Di seguito verrà descritta la
comparsa di un nuovo virus responsabile di un'epidemia di
polmonite atipica che ha coinvolto numerosi Paesi dell'Asia,
dell'America e dell'Europa. Verranno, poi, analizzate le
principali caratteristiche strutturali e saranno indicati gli
attuali strumenti diagnostici e, infine, sarà valutato il
possibile rischio trasfusionale legato alla trasmissione del
nuovo microrganismo.
La prima epidemia del XXI secolo
Sebbene la prima segnalazione ufficiale di un'epidemia
di polmonite atipica risalga all'11 febbraio 2003, i primi casi
di Severe Acute Respiratory Syndrome (SARS) si possono
far risalire alla metà del novembre 2002 nella provincia di
Guangdong nella Cina Meridionale. Nel periodo intercorso
tra la comparsa del caso indice e la segnalazione
all'Organizzazione Mondiale della Sanità (OMS), 305
soggetti si erano ammalati e 5 erano morti per la sindrome.
Circa il 30% degli infetti erano operatori sanitari, venuti a
stretto contatto con i malati. Un medico cinese che operava
in un ambulatorio nella regione di Guangdong si trasferisce,
il 21 Febbraio, ad Honk Kong e si stabilisce al nono piano
di un albergo del centro cittadino. Nei giorni successivi
almeno 12 ospiti dell'albergo manifestano i primi sintomi:
alcuni di essi vengono ricoverati al Queen Mary Hospital e
Prince of Wales Hospital di Honk Kong, altri, raggiungono
le successive tappe del loro viaggio e vengono
ospedalizzati ad Hanoi (Vietnam), Toronto (Canada) e
Singapore13,14. Rapidamente, i casi si moltiplicano
soprattutto negli operatori sanitari venuti a stretto contatto
con i malati e la sindrome si diffonde, veicolata dai
viaggiatori internazionali. Nuovi infetti vengono segnalati
ad Honk Kong, Singapore, Canada, Cina. Il 12 marzo, l'OMS
lancia la Global Alert ed il 15 marzo l'Emegency Travel
Advisory. Il numero cumulativo di casi registrati supera le
5.000 unità il 28 aprile, le 6.000 il 2 maggio, le 7.000 l'8 maggio,
con 30 nazioni in 6 continenti coinvolti dall'epidemia. Il
picco epidemico viene raggiunto la prima settimana di
maggio (Figura 1), con 1.400 casi riportati. Nelle settimane
successive, si è osservata una rapida diminuzione dei casi,
con alcune preoccupanti eccezioni rappresentate dalla Cina
continentale, da Taiwan e dal Canada, dove, dopo una fase
di controllo dell'infezione, si è assistito ad una
recrudescenza dell'epidemia. Nell'ultima settimana di giugno,
Pechino ed Hong Kong, due delle città più colpite
dall'epidemia, sono state dichiarate libere da trasmissione
217
G Icardi et al.
Figure 1 - Course of SARS epidemic (source: www.who.int)
last week of June, Peking and Hong Kong, two of the cities
most severely affected by the epidemic, were declared free
of local transmission and new cases were recorded only in
Toronto and Taiwan.
At the time of writing (September 2003), 8,098 cases
have been reported and the mortality rate, calculated by
the WHO, is 10%, although it reaches almost 50% in over
65-year olds.
Identification of the causal agent: the SARS-CoV
Since April 2000, the WHO has co-ordinated the Global
Outbreak Alert and Response Network (GOARN), an
international network fed by 112 other national or
continental networks, which collects virological,
bacteriological and epidemiological surveillance data and
unites the expertise of the international scientific community
in order to guarantee a rapid response in the case of the
risk of an epidemic. Since its creation in 1998, up to 2002,
over 500 epidemic events had been investigated in 132
countries, but rarely has GOARN and its partner networks
been required so urgently. The initial plan of intervention
was decided between March 12th and 15th and was based
on the creation of a network of 11 laboratories given the
task of identifying the agent causing SARS. On April 17th,
just one month after the constitution of the network of
laboratories, it was announced that the aetiological agent
had been identified: a new virus belonging to the
Coronavirus family15,16. A few days later, the complete
sequence of the genome of the new micro-organism was
published online in the World Wide Web.
The SARS-CoV, as the new virus was called, although
218
locale e solamente a Toronto e Taiwan vengono registrati
nuovi casi.
A tutt'oggi (settembre 2003), sono stati riportati 8.098
casi e la letalità, calcolata dall'OMS, è pari al 10%, con punte
fino al 50% nella popolazione ultrasessantacinquenne.
L'identificazione dell'agente causale: il SARS-CoV
Dall'aprile 2000, l'OMS coordina il Global Outbreak
Alert and Response Network (GOARN), una rete
internazionale, cui afferiscono altri 112 network nazionali o
continentali, in grado di raccogliere dati di sorveglianza
epidemiologica, batteriologica e virologica, e di riunire
l'epertise della comunità scientifica internazionale per
garantire una risposta rapida in caso di rischio epidemico.
Dalla fondazione nel 1998 al 2002, oltre 500 eventi epidemici
sono stati investigati in 132 Paesi, ma in poche altre
situazioni la richiesta al GOARN e ai network partner è
stata così urgente. Il piano iniziale d'intervento è stato
progettato tra il 12 ed il 15 marzo e ha visto tra i suoi punti
caratterizzanti la creazione di una rete di 11 laboratori volta
all'identificazione dell'agente causale della SARS. Il 17 aprile,
a un mese dalla costituzione del network di laboratori, viene
dato l'annuncio dell'identificazione dell'agente etiologico:
un nuovo virus appartenente alla famiglia dei
Coronavirus15,16. Alcuni giorni dopo, viene pubblicata in
rete la sequenza completa del genoma del nuovo
microrganismo.
Il SARS-CoV, come viene battezzato il nuovo virus, pur
mantenendone la struttura, è filogeneticamente lontano dai
Coronavirus isolati nell'uomo e negli altri animali e va a
costituire un cluster ben separato dagli altri tre in cui erano
Blood Transf 2003; 3: 215-23
SARS and blood transfusion
maintaining the structure of a Coronavirus, is
phylogenetically distant from the Coronaviruses isolated
in man and other animals and forms a cluster clearly distinct
from the other three in which the micro-organisms of this
family had so far been grouped17,18. Many hypotheses on
the origin of the SARS-CoV have been offered, but most
are subject of ongoing studies and only preliminary results
are available. Sequencing analysis has shown that the open
reading frames, coding for the structural and non-structural
proteins of the virus, do not resemble those of the other
Coronaviruses, which indicates that recombination
phenomena with already known viruses are improbable,
despite the fact that genetic exchange between microorganisms of this family are common and have been well
documented in the literature17-19. The new micro-organism
seems to have evolved independently, but the host in which
it accumulated its numerous mutations remains to be
discovered. This information is of fundamental importance,
not only for the phylogenetic analysis and identification of
the evolutionary mechanisms of the new micro-organism,
but above all to discover the natural reservoir, to predict
antigenic variation and therefore to be able to fine-tune the
preventive and diagnostic instruments. Preliminary studies,
presented at the recent Expert Meetings held in Kuala
Lumpur in the third week of June and in Okinawa, Japan, in
October, revealed that viruses similar to SARS-CoV have
been isolated from the Himalayan palm civet and Raccoondog, two small mammals whose natural habitat is southern
China20. Neither chicken nor pigs, key animals in the antigenic
shift of influenza viruses, seem to play and important role in
the evolution of SARS-CoV and do not seem to provide a
viral reservoir21.
The diagnostic approach and transfusion risk
The possibility of an early diagnosis and identification
of the most appropriate diagnostic instrument are
inseparably linked to physiological knowledge and
understanding of the natural history of the infection. The
lack of information about the anatomical sites and duration
of replication of SARS-CoV, the viral load in biological
fluids during the various stages of the infection and the
resistance of the micro-organism outside the host, are all
obstacles to producing diagnostic strategies. Indeed,
some aspects of the kinetics of the virus have surprised
the scientific community: unlike other viruses that
replicate in mucosa (such as the influenza orthomyxovirus)
or have air-borne transmission and double replication
(such as the measles paramyxovirus), SARS-CoV is not
Blood Transf 2003; 3: 215-23
fino ad oggi raggruppati i microrganismi di questa
famiglia17,18. Sull'origine del SARS-CoV sono state proposte
molte ipotesi, ma gran parte degli studi sono in progress e
solo i primi risultati sono disponibili. L'analisi di sequenza
ha rivelato che gli open reading frame, codificanti le
proteine strutturali e non strutturali del virus, sono distanti
da quelli degli altri Coronavirus, il che sta a indicare che
fenomeni di ricombinazione con virus ad oggi noti sono
improbabili, nonostante lo scambio genetico fra
microrganismi di questa famiglia sia frequente e ben
documentato in letteratura17-19. Il nuovo microrganismo
sembra si sia evoluto in modo indipendente, ma rimane da
scoprire in quale ospite abbia accumulato le numerose
mutazioni. Questi dati hanno un ruolo fondamentale, non
solo per l'analisi filogenetica e l'individuazione dei
meccanismi evolutivi del nuovo microrganismo, ma sono
di grande importanza per individuarne il reservoir naturale,
predirne la variazione antigenica e calibrare, quindi, gli
strumenti preventivi e diagnostici. Studi preliminari,
presentati ai recenti Expert Meetings, svoltosi a Kuala
Lumpur nella terza settimana di giugno e a Okinawa in
ottobre, hanno rivelato come virus simili al SARS-CoV siano
stati isolati nell'Himalayan palm civet e nel Raccon-dog,
due piccoli mammiferi che hanno il loro habitat nella Cina
meridionale20. Sia polli che suini, animali-chiave nello shift
dei virus influenzali, non sembrano giocare un ruolo
importante nell'evoluzione del SARS-CoV e non sembrano
rappresentare il reservoir virale21.
L'approccio diagnostico e il rischio trasfusionale
La possibilità di una diagnosi precoce e l'identificazione
dello strumento diagnostico più idoneo non possono
prescindere dalle conoscenze sulla fisiopatologia e sulla
storia naturale dell'infezione. Le lacune che ancora esistono
sui siti anatomici e sulla durata della replicazione del SARSCoV, sulla concentrazione virale nei liquidi biologici durante
le diverse fasi dell'infezione e la resistenza del microrganismo
al di fuori dell'ospite, rappresentano ostacoli per la messa a
punto di strategie diagnostiche. In particolare, alcuni aspetti
riguardo la cinetica virale hanno sorpreso la comunità
scientifica: contrariamente ad altri virus a replicazione
mucosale (quale l'orthomixovirus dell'influenza) o
caratterizzati da trasmissione aerea e duplice replicazione
(quali il paramyxovirus del morbillo), il SARS-CoV non è
eliminato in modo massivo nell'ultima fase dell'incubazione
e nei primi giorni dalla comparsa dei sintomi. I primi studi di
cinetica virale hanno permesso di rilevare il massimo
shedding intorno al 10°-12° giorno dalla comparsa dei
219
G Icardi et al.
massively eliminated in the final phase of the incubation
and during the first few days of symptoms. The early
studies of the viral kinetics revealed that maximum
shedding occurs between the 10th - 12th day after the onset
of symptoms. This fact obviously affects the detection
rate of the virus in the faeces and nasopharyngeal
aspirates, which are the substrates in which non-SARS
human Coronaviruses are eliminated. Preliminary data on
Hong Kong patients, presented by JSM Peiris at the Kuala
Lumpur conference, 22 showed that 25-45% of
nasopharyngeal swabs were positive in the first week
and 65-80% in the second week after the onset of the
symptoms22,23. The SARS-CoV was detected later in faecal
samples: in fact, it was completely absent up to the 5th-6th
day, but was found in 85% of samples between the 11th
and 16th day.
The low viral shedding in the first week following the
onset of symptoms leads to the need to produce highly
sensitive diagnostic techniques to guarantee the early
diagnosis, essential for prevention. The approaches so
far used for the diagnosis of SARS-CoV are the classical
virology methods based on direct detection of the virus
by isolation from cell cultures or molecular techniques or
detection of specific immunofluorescent antibodies. The
most promising, in terms of fast performance and high
sensitivity, are the tests based on gene amplification. The
sequencing information on the first isolates allowed the
design of primers, already available on April 17th, and
the development of nested-PCR and real-time PCR. The
need to have a sensitive and specific test as quickly as
possible spurred the effort to standardise the proposed
tests, but the process of optimisation has only just begun.
At present, the laboratory tests are only an important
complement to a diagnosis still based on clinical and
epidemiological data. In fact, following the latest WHO
indications, negative results in current diagnostic tests
do not have particular relevance for the management of a
possible SARS-CoV infection or for undertaking control
measures. The reasons for the poor predictive value of a
negative test lies in the very low viral shedding in the
first stage of the infection, in the insufficiently low
sensitivity of the PCR-based tests and in the delayed
appearance of the antibodies. The diagnostic tests must
still overcome many of these problems. The variability
and evolutionary capacity of the virus are still largely
unknown and the first studies highlight mutations in
regions that, until now, had been considered highly
conserved24. If this finding is also confirmed for the region
amplified in molecular tests, it would make current
techniques less sensitive and increase the number of false
220
sintomi. Questo dato ha naturalmente influenzato la
percentuale di rilevamento del virus nelle feci e nell'aspirato
naso-faringeo, che rappresentano i substrati in cui vengono
eliminati i Coronavirus umani non-SARS. Dati preliminari
presentati alla Conferenza di Kuala Lumpur da JSM Peiris22
sui pazienti di Hong Kong hanno mostrato positività del
25-45% dei tamponi naso-faringei nella prima settimana e
65-80% nella seconda settimana dalla comparsa dei
sintomi22,23. Il SARS-CoV è stato rilevato più tardivamente
nei campioni di feci: è risultato, infatti, completamente
assente fino al 5°-6° giorno per raggiungere la percentuale
di positivi dell'85% tra l'11° e il 16° giorno. Il basso shedding
virale nella prima settimana dalla comparsa dei sintomi
spinge alla necessità di tecniche ad elevata sensibilità al
fine di garantire una diagnosi precoce, indispensabile a fini
preventivi. Gli approcci fino ad ora impiegati per la
diagnostica del SARS-CoV sono quelli classici della
virologia e si basano sul rilevamento diretto del virus,
mediante isolamento su coltura cellulare o tecniche
molecolari o la rivelazione degli anticorpi specifici in
immunofluorescenza. Sicuramente più promettenti, per
velocità di esecuzione ed elevata sensibilità, sono i test
basati sull'amplificazione di materiale genetico. Le
informazioni sulla sequenza dei primi isolati hanno permesso
il disegno dei primers, la cui sequenza era disponibile già il
17 aprile, e la messa a punto di nested-PCR e real-time
PCR. La necessità della disponibilità al più presto di un
test sensibile e specifico ha moltiplicato gli sforzi per la
standardizzazione dei test proposti, ma il processo di
ottimizzazione è, con ogni probabilità, appena incominciato.
Attualmente, i test di laboratorio rappresentano soltanto
un importante complemento alla diagnosi, che rimane legata
a criteri clinici ed epidemiologici. Il risultato negativo agli
attuali test diagnostici non assume, infatti, seguendo le
indicazione dell'OMS e da quanto emerso dalle più recenti
revisioni, particolare significato nella gestione della
possibile infezione da SARS-CoV e nell'intraprendere le
misure di controllo. Le ragioni dello scarso valore predittivo
del test negativo vanno ricercate nello shedding virale
molto basso nella prima fase di infezione, in una sensibilità
troppo bassa dei PCR-based test e nella comparsa tardiva
degli anticorpi. Molti sono i quesiti ancora aperti e le
problematiche da affrontare in ambito diagnostico. La
variabilità e la capacità evolutiva del virus sono ancora
largamente sconosciute e i primi studi mettono un luce
mutazioni in regioni fino ad oggi ritenute molto
conservate24. Queste informazioni, se confermate per la
regione amplificata dai test molecolari, potrebbero rendere
meno sensibili le attuali tecniche ed aumentare il numero
dei falsi negativi. Inoltre, non è di facile interpretazione, sia
Blood Transf 2003; 3: 215-23
SARS and blood transfusion
negatives. Furthermore, it is not easy give a diagnostic or
epidemiological interpretation to the finding of a modest
amount of viral RNA in asymptomatic individuals or in
patients with very few symptoms25.
The finding of viral RNA, albeit in limited amounts, in
the plasma of patients in the acute phase of the disease,
raises the spectre of the risk of transmission of SARSCoV via blood or blood products26. So far, no case of
probable SARS has been attributed to this route of
transmission but, given the theoretical risk, the
Department of Blood Safety and Clinical Technology of
the WHO has issued a series of recommendations. The
recommendations for those areas, such as Italy, in which
local transmission has not occurred, electively concern
travellers arriving from infected areas. Asymptomatic
travellers should delay donation until 3 weeks after their
return; symptomatic travellers who are defined as
suspected or probable cases should delay donation for,
respectively, one or three months after the completion of
treatment and the disappearance of symptoms. These
recommendations are also valid in areas of recent local
transmission: a person in close contact with a case should
delay donation for 3 weeks, while suspected and
probable cases are subject to the same recommendations
described above (www.who.int/csr/sars). While awaiting
a highly sensitive diagnostic test for the detection of
Coronavirus in the blood and an evaluation of the
appropriateness of introducing this into blood testing,
donor selection plays an essential role. The numerous
uncertainties concerning the natural history of the
infection are reflected by the questions on the possible
role of transfusion as a method of transmission of SARSCoV. The risk assessment associated with transfusion
of blood components and plasma derivatives, which can
be defined by look back and trace back studies, presymptomatic viraemia, ex vivo stability of the virus,
protocols for the production of blood components, as
well as the use of convalescents are the current priorities
in Transfusion Medicine research26,27.
Blood Transf 2003; 3: 215-23
dal punto di vista diagnostico che epidemiologico, il
rilevamento di modeste quantità di RNA virale in soggetti
asintomatici o paucisintomatici25.
Il rilievo di RNA virale nel plasma di pazienti in fase
acuta, seppure in quantità modeste, ha proposto
all'attenzione della comunità scientifica il rischio della
trasmissione del SARS-CoV mediante sangue o
emoderivati26. A oggi, nessun caso probabile di SARS è
ascrivibile a questa modalità di trasmissione, ma in funzione
di questo rischio teorico il Department of Blood Safety
and Clinical Technology dell'OMS ha proposto una serie
di raccomandazioni. Le raccomandazioni per quelle aree,
come l'Italia, in cui non si è verificata trasmissione locale,
riguardano elettivamente i viaggiatori provenienti da aree
infette. I viaggiatori asintomatici dovranno posticipare la
donazione di 3 settimane dalla data del ritorno, i viaggiatori
sintomatici che rientrano nella definizione di caso sospetto
o probabile dovranno posticipare la donazione,
rispettivamente, di 1 mese o 3 mesi dalla cessazione della
terapia e dal termine della sintomatologia. Queste
raccomandazioni vengono riprese anche in quadri
epidemiologici caratterizzati da recente trasmissione locale:
il contatto stretto di caso dovrà posticipare la donazione di
3 settimane, mentre per i casi sospetti o probabili valgono
le indicazioni soprariportate (www.who.int/csr/sars). In
attesa di un test diagnostico ad elevata sensibilità per il
rilevamento del Coronavirus nel sangue e della valutazione
sull'opportunità dell'introduzione di un test di questo tipo
nel blood testing, la selezione del donatore gioca il ruolo
principale. Le numerose incertezze sulla storia naturale
dell'infezione si riflettono sugli interrogativi sul possibile
ruolo della trasfusione quale modalità di trasmissione del
SARS-CoV. Il risk assessment, legato alla trasfusione di
sangue di emocomponenti e di plasmaderivati, definibile
con studi look back and trace back, la viremia presintomatica, la stabilità del virus ex vivo, la valutazione del
rischio nei plasmaderivati e i protocolli per la loro
produzione, nonché l'uso dei convalescenti sono
attualmente quesiti prioritari per la ricerca in ambito
trasfusionale26,27.
221
G Icardi et al.
References
1) Woolhouse MEJ. Population biology of emerging and re-emerging pathogens. Trends in Microbiol 2002; 10: S3-S7.
2) Leport C, Janowski M, Brun-Vezinet F, et al. West Nile virus meningomyeloencephalitis—value of interferon assays in primary
encephalitis. Ann Med Intern 1984; 135: 460-3.
3) Han LL, Popovici F, Alexander JP Jr, et al. Risk factors for West Nile virus infection and meningoencephalitis, Romania,1996. J
Infect Dis 1999; 179: 230-3.
4) Mukinda VB, Mwema G, Kilundu M, et al. Re-emergence of human monkeypox in Zaire in 1996. Monkeypox Epidemiologic
Working Group. Lancet 1997; 349: 1449-50.
5) CDC. Multistate outbreak of monkeypox-Illinois, Indiana, and Wisconsin, 2003. MMWR Morb Mortal Wkly Rep 2003; 52:
537-40.
6) Scholtissek C, Burger H, Bachman PA, Hannoun C. Genetic relatedness of haemaggglutinins of the H1 subtype of influenza A
viruses isolated from swine and birds. Virology 1983; 129: 521-3.
7) Hinshaw VS, Webster RG, Turner B. Novel influenza A viruses isolated from Canadian feral ducks: including strain antigenically
related to swine influenza (Hsw1N1) viruses. J Gen Virol 1978; 41: 115-27.
8) Guo Y, Wang M, Kawaosoka Y, et al. Characterization of a new avian-like influenza A viruses from horses in China. Virology 1992;
188: 245-55.
9) Scholtissek C, Burger H, Kistner O, Shortridge KF. The nucleoprotein as a possible major factor in determining host specificity
of influenza H3N2 viruses. Virology 1985; 147: 287-94.
10) Scholtissek C. Pigs as "mixing vessels" for the creation of new pandemic influenza A viruses. Med Principles Pract 1990; 2: 6571.
11) Chan PK. Outbreak of avian influenza A(H5N1) virus infection in Hong Kong in 1997. Clin Infect Dis 2002; 34: S58-64.
12) Lin YP, Shaw M, Gregory V, et al. Avian-to-human transmission of H9N2 subtype influenza A viruses: relationship between
H9N2 and H5N1 human isolates. Proc Natl Acad Sci USA 2000; 97: 9654-8.
13) Tsang KW, Ho PL, Ooi G, et al. A cluster of cases of Severe Acute Respiratory Syndrome in Hong Kong. N Engl J Med 2003; 348:
1977-85.
14) Poutanen SM, Low DE, Henry B, et al. Identification of Severe Acute Respiratory Syndrome in Canada. N Engl J Med 2003; 348:
1995-2005.
15) Ksiatek TG, Erdman D, Gordsmith C, et al. A novel Coronavirus associated with Severe Acute Respiratory Syndrome. N Engl
J Med 2003; 348: 1947-58.
16) Drosten C, Gunther S, Preiser W, et al. Identification of a novel Coronavirus in patients with Severe Acute Respiratory Syndrome.
N Engl J Med 2003; 348: 1667-76.
17) Marra MA, Jones SJM, Astell CR, et al. The genome sequence of the SARS-associated Coronavirus. Science 2003; 300: 1399404.
18) Rota PA, Oberste MS, Monroe SS, et al. Characterization of a novel Coronavirus associated with Severe Acute Respiratory
Syndrome. Science 2003; 300: 1394-9.
19) Lai MMC. RNA recombination in animal and plant viruses. Microbiol Rev 1992; 56: 61-79.
20) Guan Y, Zheng BJ, Shortridge KF, et al. Isolation and characterization of viruses related to SARS Coronavirus from animals in
Southern China. Personal Communication in WHO Global Conference on Severe Acute Respiratory Syndrome. Kuala Lumpur,
Malaysia, 17-18 June 2003.
21) Weirgartl H, Copps J, Drebot M, et al. Susceptibility of pigs and chickens to SARS Coronavirus. Personal Communication in
WHO Global Conference on Severe Acute Respiratory Syndrome. Kuala Lumpur, Malaysia, 17-18 June 2003.
22) Peiris JSM. SARS: aetiology. Personal Communication in WHO Global Conference on Severe Acute Respiratory Syndrome.
Kuala Lumpur, Malaysia, 17-18 June 2003.
23) Peiris JSM, Chu CM, Cheng VCC, et al. Clinical progression and viral load in a community outbreak of Coronavirus associated
SARS pneumonia: a prospective study. Lancet 2003; 361: 1767-71.
24) Ruan YJ, Wei CL, Ee AL, et al. Comparative full-length genome sequence analysis of 14 SARS Coronavirus isolates and common
mutations associated with putative origins of infection. Lancet 2003; 361: 1779-86.
222
Blood Transf 2003; 3: 215-23
SARS and blood transfusion
25) WHO SARS Team. SARS laboratory diagnosis. Personal Communication in WHO Global Conference on Severe Acute Respiratory
Syndrome. Kuala Lumpur, Malaysia, 17-18 June 2003.
26) Dhingra N. SARS as an emerging pathogen: implications for blood safety. Personal Communication in WHO Global Conference
on Severe Acute Respiratory Syndrome. Kuala Lumpur, Malaysia, 17-18 June 2003.
27) Lloyd N. Blood safety – WHO strategies. Personal Communication in: The impact of SARS and other emerging pathogens on
transfusion medicine. Brussels, Belgium, 16 June 2003.
Blood Transf 2003; 3: 215-23
223