Year 1 ı Number 4 ı 2015
205
USEFULNESS OF TREHALOSE FOR CONTACT LENS WEARERS
Utilità di trealosio nei portatori di lenti a contatto
Claudia Guarracino
Head of Asso Vision Contactology Group
Salus Private Hospital - Battipaglia (Sa)
INTRODUCTION
Management of contact lens
discomfort (CLD) represents the
contactologist’s primary daily
challenge. It is estimated that there are
currently over 140 million contact lens
wearers in the world and studies have
recorded a 12% to 51% discontinuation
rate with the primary reason given as
contact lens discomfort1-2. However, up
until recent years, little consensus on
the definition of CLD existed.
The Tear Film and Ocular Surface
Society’s (TFOS) 2013 Workshop
Report on Contact Lens Discomfort
made an important contribution in
this regard, defining it as a condition
characterised by episodic or persistent
adverse ocular sensations connected
to lenses, with or without visual
disturbances, resulting from reduced
compatibility between the contact
lenses and the ocular area, which
may lead to reduced wearing time
and permanent discontinuing use of
contact lenses1. In naïve contact lens
wearers, the discomfort develops
after an initial adaptation phase and
becomes more intense when the
contact lenses are worn. Typically,
removal of the contact lenses mitigates
symptoms1. Published works often
make a connection between CLD and
dry eye. In fact, dry eye syndrome
affects 35%-60% of contact lens
INTRODUZIONE
La gestione del discomfort da lente a
contatto (CLD) rappresenta la principale
sfida che il contattologo si trova
quotidianamente ad affrontare. Si stima
che attualmente ci siano più di 140 milioni
di portatori di lenti a contatto (LAC) in tutto il
mondo e gli studi riportano una percentuale
di abbandono delle LAC compreso
tra il 12% e il 51%, riconoscendo nel
discomfort da lente a contatto il principale
motivo di abbandono1-2.
Ma fino a qualche anno fa c’è stato
poco consenso sulla definizione di CLD.
Nel 2013 il report del TFOS (Tear Film
and Ocular Surface Society) Workshop
sul Discomfort da LAC ha dato un
importante contribuito in tal senso,
definendolo una condizione caratterizzata
da episodiche o persistenti sensazioni
oculari avverse legate alla lente, con o
senza disturbi visivi, derivante da ridotta
compatibilità tra la lente a contatto ed
ambiente oculare, che può condurre
ad un ridotto tempo di applicazione ed
abbandono definitivo delle LAC1.
Nel nuovo portatore di LAC il discomfort
si sviluppa dopo un’iniziale fase di
adattamento e diventa più intenso
quando la LAC viene indossata. In
genere, la rimozione della LAC mitiga i
sintomi1..
In letteratura viene spesso fatta una
associazione tra CLD e occhio secco,
infatti la secchezza oculare colpisce
The author declares that
there are no conflicts of
interest in relation to this
article
CORRESPONDING
AUTHOR
Claudia Guarracino
[email protected]
KEY WORDS
CLD (contact lens
discomfort), keratoconus,
Ferning test, tear substitutes, trehalose
PAROLE CHIAVE
CLD (discomfort da lente
a contatto) , cheratocono,
test difelcizzazione, sostituti
lacrimali, trealosio
206
Usefulness of trehalose for contact lens wearers
wearers and is, in turn, considered the
most common cause of contact lens
discontinuation in the medium and
long term2. However, The TFOS Report
stresses the need to differentiate
between the terms "dry eye linked to
contact lenses" and “CLD”, highlighting
that the former should only refer to
patients with a pre-existing dry eye
condition that can be aggravated
by the use of contact lenses1. It is,
nonetheless, still a fact that contact
lens / tear film interaction plays a
crucial role in provoking discomfort.
In fact, the available evidence points
to an association between lenses
and tear film instability, increased tear
evaporation, reduced tear film turnover
and altered tear ferning1. In 1971, Holly
attributed contact lens-related tear
evaporation to a process of water
evaporation from the precorneal tear
film: the aqueous layer decreases
leading to precipitation through which
the lipid layer can contaminate the
mucous layer of the corneal epithelium
microvilli3. This involves the inactivation
of the mucin’s hydrophobic function
with the subsequent formation of
hydrophobic zones (dry spots). This
suggests that by integrating the
lipid layer, lipid degradation could
be slowed, making it possible to
stabilise the other two layers. It is
possible to identify tear film stability
as being a key factor in CLD, but the
link between CLD and damage to
the ocular surface (corneal staining
test) is less obvious, while greater
attention is focused on changes in
Meibomian gland function1. Patients
with keratoconus can use soft contact
lenses in the early stages. However,
as the disease progresses, the cornea
becomes more irregular and patients
must switch to a rigid gas permeable
lenses (RGP lenses)4-5. In cases of
il 35-60% dei portatori di LAC ed è
a sua volta ritenuta la più importante
causa di abbandono di LAC a medio
e lungo termine2. Tuttavia nel report
del TFOS si sottolinea la necessità di
differenziare i termini “occhio secco
correlato a LAC” dalla CLD, riservando
il primo solo ai pazienti con preesistente
condizione di secchezza oculare che
può essere aggravata dall’uso delle
LAC1. È comunque assodato che
l’interazione LAC/film lacrimale abbia un
ruolo cruciale nella genesi del discomfort,
infatti le evidenze disponibili lo associano
a diminuita stabilità del film lacrimale,
aumentata evaporazione lacrimale, ridotto
turnover del film lacrimale ed alterata
felcizzazione1. Già Holly nel 1971, attribuì
la dislacrimia da LAC ad un processo di
evaporazione dell’acqua dal film lacrimale
precorneale: lo strato acquoso diminuisce
ed i lipidi dello strato superficiale possono
contaminare, per precipitazione, lo strato
mucoso che ricopre i microvilli dell’epitelio
corneale3. Ciò comporta l’inattivazione
della funzione idrofilizzante della mucina
con conseguente formazione di zone
idrofobe (dry spots). Se ne deduce
dunque che se si riesce ad integrare lo
strato lipidico, rallentando la degradazione
lipidica, questo ci consentirebbe di
stabilizzare anche gli altri due strati. Se la
stabilità del film lacrimale ha un ruolo di
fattore chiave nella CLD, meno evidente
risulta il nesso tra CLD e danno alla
superficie oculare (test di colorazione
corneale), mentre maggiore attenzione
è riservata alle modificazioni palpebrali
per la funzionalità delle ghiandole
di Meibomio1. Nei pazienti affetti da
cheratocono si possono utilizzare
lenti a contatto morbide regolari negli
stadi iniziali. Con la progressione della
malattia, la cornea diventa più irregolare
e occorre ricorrere ad una lente rigida
gas permeabile (LAC-RGP)4-5. Nei casi
di cheratocono avanzato, cui venga
Year 1 ı Number 4 ı 2015
207
Utilità di trealosio nei portatori di lenti a contatto
advanced keratoconus, where RGP
lenses are prescribed, there is usually
a higher incidence of tear evaporation.
In fact, the effects of contact lenses on
lacrimal function adds to the negative
impact of keratoconus which, due to
the irregular ocular surface, interferes
with homogeneous distribution and
integrity of the lipid layer due to poor
lid congruity, abnormal eyelid dynamics
and low blink rate.
Published works cite that
approximately 80% of cases of
contact lens intolerance in keratoconus
is attributed to alterations of the
tear film6-8. Therefore, RGP lenses
application becomes more challenging
for these patients. Beyond the corneal
contact lens conformity, there are also
increased risks of complications such
as abrasions, chemosis and corneal
edema, although none of this should
affect the probability of therapeutic
success and benefits of better visual
acuity when compared to glasses9.
The key message from the TFOS
Workshop is, therefore, even more
compelling for those who wear RGP
lenses for keratoconus: "the prevention
and management of CLD should
begin at the earliest possible moment,
even before the onset of symptoms,
to improve long-term satisfaction,
safety and comfort in wearing contact
lenses"1. In contactologist practice, it is
essential to evaluate the tear film prior
to prescribing any type of contact lens.
This is best done using straightforward
tests such as Break Up Time (B.U.T.),
which documents the stability of the
tear film, the Schirmer Test which
measures the aqueous layer, and the
Ferning Test which records mucin
layer quality. The results of these tests
are often correlated: for example, a
reduced B.U.T. is often linked to a
low-level Schirmer Test and an even
prescritta una LAC-RGP si riscontra
abitualmente una maggiore incidenza di
dislacrimia, infatti agli effetti della LAC
sulla funzione lacrimale si aggiunge
l’impatto negativo del cheratocono che, a
causa della superficie oculare irregolare,
interferisce su omogeneità di distribuzione
ed integrità dello strato lipidico per
scarsa congruità palpebrale, alterazione
della dinamica palpebrale e riduzione
dell’ammiccamento. In letteratura circa
l’80% dei casi di intolleranza alla LAC nel
cheratocono è attribuita ad alterazioni del
film lacrimale6-8. Pertanto in questi pazienti
l’applicazione di una LAC-RGP diventa
più impegnativa, anche a prescindere
dalla corneoconformità della lente, con
maggior rischio di complicazioni come
abrasioni, chemosi ed edemi corneali,
anche se ciò non pregiudica a priori le
probabilità di successo terapeutico ed
i benefici di una migliore acuità visiva
rispetto agli occhiali9. Pertanto, nei
portatori LAC-RGP per cheratocono il
messaggio chiave del TFOS Workshop
è ancora più cogente: “la prevenzione
e gestione del CLD deve iniziare al
più presto, forse ancor prima della
comparsa dei sintomi, per migliorare
la soddisfazione a lungo termine, la
sicurezza e il comfort nell’indossare
la LAC”1. Nella pratica contattologica
prima di prescrivere qualunque tipo di
LAC, è indispensabile la valutazione
del film lacrimale mediante test di facile
esecuzione come il Break up time
(B.U.T.) che documenta la stabilità del
film lacrimale, il test di Schirmer che
misura l'entità dello strato acquoso, ed
il test di felcizzazione che documenta
la qualità dello strato mucinico. I risultati
di tali test sono spesso correlati, ovvero
ad un B.U.T. ridotto spesso si associa
uno Schirmer test scarso ed un test di
felcizzazione peggiore. In particolare il
test di felcizzazione, riflette le condizioni
del muco ed indirettamente fornisce
208
Usefulness of trehalose for contact lens wearers
lower level Ferning Test. In particular,
the Ferning Test, which reflects mucus
condition, can indirectly also provide
indications on tear osmolarity. Ferning
Test usefulness in predicting ability
to tolerate contact lenses was first
described by Kogbe and Liotet10.
Ravazzoni et al. demonstrated that
Type I and II of the Ferning Test
(where Type I indicates the highest
level of mucus and tear film efficiency
while Type IV the lowest), before
applying contact lenses function as
good indicators of future contact lens
tolerance, with a sensitivity rating
of 57.9% and a specificity rating of
88.5%11.
In contact lens management, primary
attention should be focused on
factors closely related to the lenses
(type and composition, signs of
deterioration, solution). Using artificial
tears regularly throughout the day
also plays a significant role in relieving
symptoms12-14.
Recent evidence supports the
hypothesis that new trehalose-based
eye-drops can be useful in contact
lens management, by protecting
the corneal epithelium in particular
environmental conditions which
contact lens wearers experience.
Moreover, these drops have
cytoprotective properties and cell
membrane stabilisation functions,
which prevent the protein denaturation
and lipid degradation15. The product’s
non-viscosity finally allows for optimal
distribution in the tear film and a high
pass rate between the tear-film/lens
interface.
In our centre, patients usually undergo
both preventive controls using tear film
function tests (B.U.T., Schirmer and
Ferning) before contact lenses are
prescribed, and follow-up visits. If there
is evidence of CLD, then artificial tear
indicazioni anche sulla osmolarità delle
lacrime. L’utilità predittiva del test di
felcizzazione per la tollerabilità delle LAC
fu descritta per la prima volta da Kogbe
e Liotet10. Ravazzoni et al. dimostrarono
poi che il tipo I e II di questo test
(laddove il tipo I indica una migliore
efficienza del muco e del film lacrimale,
mentre il tipo IV la peggiore), prima di
indossare LAC, possono essere utilizzati
come predittivi di buona tollerabilità alla
LAC con una sensibilità del 57,9% e una
specificità del 88,5%11.
Nella gestione del CLD viene
raccomandata primaria attenzione
ai fattori strettamente correlati alla
lente (tipologia e composizione,
segni di deterioramento, soluzione
di conservazione). Riveste un ruolo
altrettanto importante anche l’uso
di lacrime artificiali che consentono
di alleviare i sintomi se utilizzate
regolarmente nell’arco della giornata12-14.
Recenti evidenze supportano l’ipotesi
che un nuovo collirio a base di trealosio
possa essere utile nella gestione del
CLD perché protegge l’epitelio corneale
in condizioni ambientali particolari,
analoghe a quelle che si realizzano in
un portatore di lenti a contatto. Inoltre
ha proprietà citoprotettive e stabilizzanti
delle membrane cellulari, impedendo
la denaturazione delle proteine e
la degradazione dei lipidi15. La non
viscosità del prodotto ne consente infine
un’ottimale distribuzione nel film lacrimale
ed un elevato passaggio nell’interfaccia
cornea-lente. Nel nostro centro i pazienti
vengono abitualmente sottoposti sia
ad accertamenti preventivi con test di
funzionalità del film lacrimale (B.U.T.,
test di Schirmer e test di felcizzazione)
prima di prescrivere le LAC sia a visite
di follow-up nelle settimane successive.
In presenza di evidenza di CLD viene
anche valutata l’opportunità di sostituire
la lacrima artificiale. Per questo motivo
Year 1 ı Number 4 ı 2015
209
Utilità di trealosio nei portatori di lenti a contatto
substitution can be considered.
For this reason it was considered
opportune to evaluate the effectiveness
of trehalose 3% eye drops in patients
using RGP lenses for keratoconus
with evidence of CLD, notwithstanding
regular use of a tear substitute.
MATERIALS AND METHODS
Patients who were selected for this
study had advanced keratoconus and
had been wearing RGP lenses for
over three months. Selected patients
had displayed signs of CLD with tear
evaporation at their check-up. This
was pinpointed through alteration in
at least two tear film function tests
(B.U.T., Schirmer Test and Ferning
Test) associated with insufficient
maximum time for the use of contact
lenses/day (< 4 hours) in spite of
regular instillation of a tear substitute
4 times/day.
All patients treated at the Contactolgy
Centre in Salus Private Hospital in
Battipaglia (SA) who matched the
aforementioned inclusion criteria
participated in this open study wherein
the tear substitute in use would be
replaced with trehalose 3% eye drops to
be applied 4 times /day for 8 weeks.
At the baseline visit (before replacing
the artificial tear solution), all patients
underwent a B.U.T. examination,
Schirmer Test and Ferning Test. In
addition, data was collected on the
maximum number of hours/day contact
lenses were worn for the 3 days prior to
the visit and patients’ overall degree of
satisfaction with wearing contact lenses
(verbal scale 0-5).
This data collection was repeated for
all patients after 8 weeks of trehalose
treatment. In some cases, it was
possible to carry out an interim checkup after 20 days. The Ferning Test
was carried out by taking tear samples
abbiamo ritenuto utile valutare l’efficacia
di un collirio a base di trealosio 3%
in pazienti portatori di LAC-RGP per
cheratocono con evidenza di CLD,
malgrado il regolare utilizzo di un sostituto
lacrimale a base di un sostituto lacrimale.
MATERIALI E METODI
Sono stati selezionati per questo studio
pazienti affetti da cheratocono avanzato,
portatori di LAC-RGP da oltre 3 mesi
che alla visita di controllo presentavano
CLD con segni di dislacrimia, definiti
dall'alterazione di almeno due test di
funzionalità del film lacrimale (B.U.T.,
test di Schirmer e test di felcizzazione)
e associati ad un tempo massimo di
utilizzo delle LAC insufficiente (≤ 4 ore/die)
malgrado la regolare istillazione di un
sostituto lacrimale applicato 4 volte/
die. A tutti i pazienti seguiti presso il
centro di contattologia della Casa di
cura SALUS di Battipaglia (SA) che
soddisfavano i suddetti criteri di inclusione
è stato proposto di partecipare a questo
studio in aperto in cui era previsto di
rimpiazzare il sostituto lacrimale in uso
con un collirio a base di trealosio 3% da
istillare 4 volte al giorno per 8 settimane.
Alla visita di selezione (prima della
sostituzione della lacrima artificiale) tutti
i pazienti sono stati sottoposti a B.U.T.,
test di Schirmer e test di felcizzazione
con rilevazione del numero massimo di
ore al giorno di utilizzo delle LAC-RGP
nei 3 giorni precedenti la visita e del
giudizio globale del paziente sul grado
di soddisfazione nell’indossare le lenti a
contatto (con una scala verbale da 0
a 5). Tali rilevazioni sono state ripetute
in tutti i pazienti dopo 8 settimane di
trattamento con trealosio, in alcuni casi è
stato possibile effettuare anche una visita
di controllo intermedia dopo 20 giorni.
Per il test di felcizzazione si è effettuato
un prelievo di lacrime (non traumatico
con una micropipetta), lasciate poi ad
210
Usefulness of trehalose for contact lens wearers
Tab.
1
Classification for Ferning Test(3)
CLASSIFICAZIONE PER TEST DI FELCIZZAZIONE(3)
Classification
Type I
Type II
Type III
Type IV
Description
Totally uniform and closely branching arborisation. Single, large,
tightly branched ferns.
Arborizzazione uniforme in tutto il campo di osservazione, senza
spazi tra le felci. Felci singole grandi e strettamente ramificate
Abundant ferning, but smaller, single ferns with less branching
than Type I; Presence of empty spaces between the ferns.
Arborizzazione abbondante, ma singoli felci più piccole con una
frequenza inferiore di ramificazione rispetto al tipo I; presenza di
spazi vuoti tra le felci
Small single ferns which are incomplete with almost no
branching.
Felci singole poco e non completamente formate con rare o
nessuna ramificazione
No ferns present; Clusters or strands of mucus may be present.
Nessuna felce presente; il muco può apparire in grappoli e filamenti
(non-traumatic technique utilising a
micropipette).
The samples were left to dry at room
temperature on a glass slide.
The samples were then studied using
a biological microscope with 4x digital
zoom to observe the characteristic
crystallisation pattern of the fern tear
and attributed a score according to
the Four-Type Grading proposed by
Rolando in 198416 defined by branching
type as described in Table 1.
RESULTS
Thirty-one adult patients with CLD
(mean age 34 years) and signs of
tear evaporation participated in
the study. All participants were
already receiving treatment with a
carboxymethylcellulose-based tear
substitute (4 instillations/day). Table
2 summarises the qualitative and
quantitative composition of the tear
film and signs of the patients’ ocular
discomfort (degree of satisfaction
essiccare su un vetrino a temperatura
ambiente. Il preparato è stato quindi
osservato con un microscopio biologico
a 4 ingrandimenti per rilevare le
caratteristiche della cristallizzazione delle
lacrime in forma di felci ed attribuire un
punteggio secondo la classificazione in
4 tipi proposta da Rolando nel 198416 in
funzione del tipo di ramificazione come
descritto in tabella 1.
RISULTATI
Hanno partecipato allo studio 31 pazienti
adulti (età media di 34 anni) con CLD e
segni di dislacrimia già tutti in trattamento
con un sostituto lacrimale a base di
carbossimetilcellulosa (4 instillazioni/
die). In tabella 2 sono riepilogate sia le
caratteristiche qualitative e quantitativa
del film lacrimale sia i segni di
discomfort oculare del paziente (grado
di soddisfazione e tempo massimo
giornaliero di utilizzo LAC) rilevate alla visita
di basale. Al termine delle otto settimane di
Year 1 ı Number 4 ı 2015
211
Utilità di trealosio nei portatori di lenti a contatto
Tab.
2
Parameters observed at the initial visit (Baseline) and the final visit (after 8 weeks)
PARAMETRI OSSERVATI ALLA VISITA INIZIALE (BASALE) E VISITA FINALE (DOPO 8 SETTIMANE)
Participant (31 Patients)
Partecipanti (31 Pazienti)
Baseline visit [mean ± SD]
VISITA basale [media ± DS]
Final visit [mean + SD]
VISITA finale [media ± DS]
B.U.T. (sec)
7,0 (±1,9)
13 (±2,4)
SCHIRMER TEST (mm)
10 (±2,8)
15 (±3,4)
FERNING TEST
(Patient distribution
for Type I to IV)
Test FELCIZZAZIONE
(distribuzione pazienti
per Tipo da I a IV)
Type I
Type II
Type III
(n 0)
(n 0)
(n13)
Type I (n14)
Type II (n17)
Type III (n 0)
Type IV
(n18)
Type IV (n 0)
Max contact lenses
wearing time (hours/day) 3,5 (±0,4)
Tmax di utilizzo LAC (ore/die)
8 (±1,4)
Patient satisfaction
score (0-5)
Giudizio del Paziente
punteggio (da 0 a 5)
4,5 (±1,4)
0,5 (±0,3)
and maximum daily contact lens
usage) which were recorded at the
baseline visit.
At the end of the eight-week
trehalose eye drop treatment, a clear
improvement of all the quantitative
parameters of the tear film was
observed. These parameters on
average indicated a decrease to within
normal limits. Moreover, tear film
stability was significantly improved,
with an increase of the average values
of the B.U.T. from baseline 7 seconds
to 13 seconds at the final visit (+ 85%).
Schirmer test average value increased
from 10 mm at the baseline at the
baseline visit to 15 mm at the final
measurement (+ 50%).
The Ferning Test was significantly
improved in all patients from Type III
or IV at the baseline to Type I or II at
the final visit. Even the maximum time
of daily use of the lenses increased
significantly, rising from 3.5 hours/day
reported at baseline to a mean of 8
trattamento con il collirio a base di trealosio
si è osservato un netto miglioramento di
tutti i parametri quali-quantitativi del film
lacrimale che sono mediamente rientrati
nei limiti di normalità, infatti la stabilità del
film lacrimale è risultata significativamente
migliorata, con un aumento dei valori medi
del B.U.T. da 7 secondi della rilevazione
basale a 13 secondi di quella finale (+85%),
il test di Schirmer è contestualmente
incrementato da un valore medio di 10 mm
al basale ai 15 mm della rilevazione finale
(+50%). Il test di felcizzazione che era stato
classificato di tipo III o IV in tutti i pazienti alla
visita basale è significativamente migliorato
con una classificazione di tipo I o II alla
visita finale in tutti i pazienti. Anche il tempo
massimo giornaliero di utilizzo delle lenti è
significativamente incrementato passando
dalle 3,5 ore/die riferite alla visita basale
ad una media di 8 ore/die riferite a quella
finale (+129%), analogamente a quanto
osservato per il giudizio globale sul grado
di soddisfazione nell’indossare le lenti a
contatto passato da un valore medio iniziale
212
Usefulness of trehalose for contact lens wearers
Fig. 1
Fig. 2
hours/day at the final visit (+ 129%).
Similarly, the overall evaluation on
the degree of satisfaction in wearing
contact lenses moved from an initial
average of 0.5 to a final rating of 4.5
(Table 2).
di 0,5 ad uno finale di 4,5 (Tab. 2).
Di seguito vengono descritte le evidenze
individuali riscontrate in alcuni pazienti
con particolare riferimento alle immagini
dei test di felcizzazione.
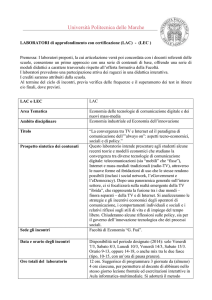
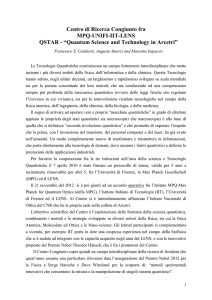
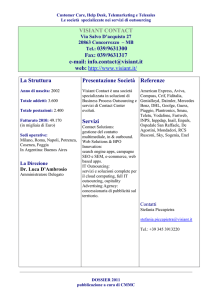
Fig. 1- 2
Ferning Test Case No. 1
Test di felcizzazione
del caso n. 1 descritto
CASE NO. 1 (RGP contact lens
wearer for Keratoconus OO) diagnosed
with lipid, aqueous and mucin layer
alterations, at baseline visit: B.U.T. =
9 sec, Schirmer Test = 10 mm, Max.
contact lens usage = 3 hours/day,
Ferning Test = Type IV (Fig. 1). Results
after 20 days of trehalose 3% treatment
3 times/day showed improvement:
B.U.T. = 12 sec, Schirmer Test = 15
mm, Max. contact lens usage = 6
hours/day, Ferning Test = Type III
(Fig. 2).
It is worth noting the remarkable
improvement after 20 days of treatment
particularly in the rate of daily usage of
contact lenses.
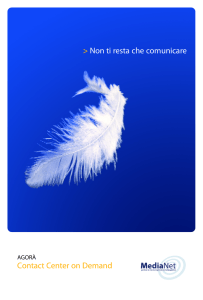
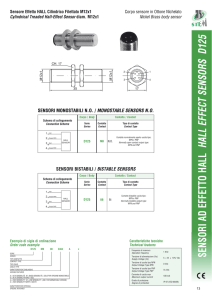
CASE NO. 2 (RGP contact lens wearer
for Keratoconus OO) diagnosed with lipid,
aqueous and mucin layer alterations, at
baseline visit: B.U.T. = 7 sec, Schirmer
Test = 10 mm, Max. contact lens usage
= 4 hours/day (not continuous), Ferning
Test = Type IV (Fig. 3). Results after 20
days of trehalose 3% treatment 3 times/
day showed improvement: B.U.T. =
CASO N. 1 portatore di LAC-RGP per
cheratocono in OO con diagnosi di
alterazione dello strato lipidico, acquoso
e mucinico alla visita basale (B.U.T. =
9 sec, Schirmer test = 10 mm, T max
di utilizzo LAC = 3 ore/die, test di
felcizzazione = IV stadio) (Fig. 1), che si è
risolta dopo 20 giorni di trattamento con
trealosio al 3% 3/die (B.U.T. = 12 sec,
Schirmer test = 15 mm, T max di utilizzo
LAC = 6 ore/die, test di felcizzazione
= III stadio) (Fig. 2) .
Da notare come dopo 20 giorni di
trattamento i parametri abbiamo avuto
un notevole miglioramento, soprattutto
il tempo di applicazione delle lenti a
contatto.
CASO N. 2 portatore di LAC-RGP per
cheratocono in OO con diagnosi di
alterazione dello strato lipidico, acquoso e
mucinico alla visita basale (B.U.T. = 7 sec,
Schirmer test = 10 mm, T max di utilizzo
LAC = 4 ore/die non continuativamente,
test di felcizzazione
= IV stadio) (Fig. 3) che si è risolta
dopo 20 giorni di trattamento con
trealosio al 3% 3/die (B.U.T. = 13
Year 1 ı Number 4 ı 2015
213
Utilità di trealosio nei portatori di lenti a contatto
Fig. 3
Fig. 4
Fig. 3-4
Ferning Test Case No. 2
Test di felcizzazione del
caso n. 2 descritto
13 sec, Schirmer Test = 15 mm, Max.
contact lens usage = 8 hours/day,
Ferning Test = Type II (Fig. 4).
This case also demonstrates that due to
the B.U.T. increase a state of equilibrium
in the layers was significant enough to
permit a great increase in the hours of
contact lens use. Most notable is the
presence of ferning in Figure 4 compared
to Figure 3 where it is completely absent.
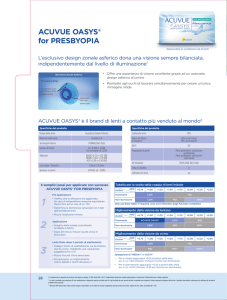
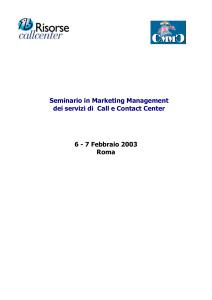
CASE NO. 3 (RGP contact lens wearer
for Keratoconus OO) diagnosed with
lipid and mucin layer alterations, at
baseline visit: B.U.T. = 8 sec, Schirmer
Test = 15 mm, Max. contact lens
usage = 3 hours/day, Ferning Test =
Type IV (Fig. 5). Results after 20 days
of trehalose 3% treatment 3 times/day
showed improvement: B.U.T. = 11 sec,
Schirmer Test = 20 mm, Max. contact
lens usage = 7 hours, Ferning Test =
Type II-III (Fig. 6).
In this case, although the patient had
a good quantity of aqueous portion
(Schirmer Test 15 mm) before the
treatment, there was, nonetheless, low
usage at only 3 hours due to immediate
evaporation as B.U.T. is only 8 seconds.
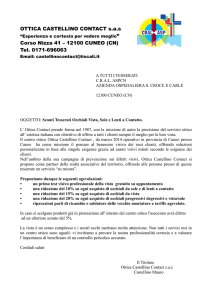
CASE NO. 4 (RGP contact lens
wearer for Keratoconus OO) diagnosed
with lipid, aqueous and mucin layer
alterations, at baseline visit: B.U.T. =
sec, Schirmer test = 15 mm, T max
di utilizzo LAC = 8 ore/die, test di
felcizzazione = II stadio) (Fig. 4) . Anche
in questo caso, grazie all’aumento del
B.U.T., si è arrivati ad una condizione di
equilibrio degli strati tale da consentire
al paziente di aumentare notevolmente
le ore di utilizzo delle LAC. Da notare
soprattutto la presenza felcizzazione nella
figura 4 rispetto alla figura 3 dove è
completamente assente.
CASO N. 3 portatore di LAC-RGP
per cheratocono in OO con diagnosi
di alterazione dello strato lipidico e
mucinico alla visita basale (B.U.T. = 8
sec, Schirmer test = 15 mm, T max
di utilizzo LAC = 3 ore/die, test di
felcizzazione = IV stadio) (Fig. 5) che si è
risolta dopo 20 giorni di trattamento con
trealosio al 3% 3/die (B.U.T. = 11 sec,
Schirmer test = 20 mm, T max di utilizzo
LAC = 7 ore, test di felcizzazione = II-III
stadio) (Fig. 6).
In questo caso nonostante il paziente
prima del trattamento avesse una buona
quantità di porzione acquosa (Schirmer
test 15 mm), l’applicazione risulta ridotta
a sole 3 ore poiché ha una evaporazione
immediata visto che il B.U.T. è di soli 8
secondi.
CASO N. 4 portatore di LAC-RGP per
cheratocono in OO con diagnosi di
214
Usefulness of trehalose for contact lens wearers
Fig. 5
Fig. 6
8 sec, Schirmer Test = 5 mm, Max.
contact lens usage = 4 hours/day,
Ferning Test = Type III (Fig. 7). Results
after 20 days of trehalose 3% treatment
3 times/day showed improvement:
B.U.T. = 12 sec, Schirmer Test = 10
mm, Max. contact lens usage = 8
hours, Ferning Test = Type I (Fig. 8).
In this case, the slide image shows
continued ferning, typical of normal tear
liquid and even though the Schirmer
Test results are not ideal, the patient is
able to wear contact lenses for 8 hours
without any discomfort.
alterazione dello strato lipidico, acquoso
e mucinico alla visita basale (B.U.T. =
8 sec, Schirmer test = 5 mm, T max
di utilizzo LAC = 4 ore/die, test di
felcizzazione = III stadio) (Fig. 7) che si è
risolta dopo 20 giorni di trattamento con
trealosio al 3% 3/die (B.U.T. = 12 sec,
Schirmer test = 10 mm, T max di utilizzo
LAC = 8 ore, test di felcizzazione = I
stadio). In questo caso l’immagine del
vetrino (Fig. 8) ci mostra una felcizzazione
continua, classica di un liquido lacrimale
normale e nonostante lo Schirmer test
non sia nei valori ideali, il paziente riesce
ad applicare le LAC per 8 ore senza
alcun fastidio.
Fig. 5-6
Ferning test Case No. 3
Test di felcizzazione del
caso n. 3 descritto
DISCUSSION AND CONCLUSIONS
It has been well-established that the
main obstacle to wider contact lens
use is the discomfort often associated
with marginal dry eye – considered the
leading cause of contact lens use being
discontinued. The Dry Eye Investigation
Study17 in the US and Canada used
a questionnaire to interview 1,054
people. Results showed that contact
lens wearers reported more frequent
symptoms of ocular discomfort,
dryness, irritation, foreign body
sensation and discomfort compared
to non-wearers. Approximately 50% of
contact lens wearers reported signs
of dryness in the evening, from mild
to severe, compared to 22% of nonwearers. In addition, 172 former contact
DISCUSSIONE E CONCLUSIONI
È ormai assodato che il principale ostacolo
alla diffusione delle lenti a contatto è il
discomfort spesso associato ad occhio
secco marginale, ritenuto la principale
causa di abbandono delle LAC.
Il Dry Eye Investigation Study17 mediante
un questionario utilizzato in USA e
Canada per intervistare 1054 soggetti, ha
evidenziato che i portatori di LAC riportano
più frequentemente sintomi di discomfort
oculare, secchezza, irritazione, sensazione
di corpo estraneo e fastidio rispetto ai
non portatori. Circa il 50% dei portatori di
LAC accusa segni di secchezza alla sera,
di intensità da lieve ad elevata, rispetto
al 22% dei non portatori. In più, 172 ex
Year 1 ı Number 4 ı 2015
215
Utilità di trealosio nei portatori di lenti a contatto
Fig. 7
Fig. 8
Fig. 7-8
Ferning Test Case No. 4
Test di felcizzazione del
caso n. 4 descritto
lens wearers stated that the two main
reasons for discontinuing use were dry
eye and ocular discomfort at the end of
the day17.
In reality, the discomfort should be
tackled as a multifactorial problem, as it
can stem from a range of factors from
optical correction, to issues relating to
the eye’s physiology and biochemistry.
Consider, for example, how lens comfort
can be substantially influenced by the
right correction to the refractive aspect.
Other important factors may be due
to reduced oxygenation, the formation
of deposits, by the mechanical action
of the lenses, from poor lens cleaning
or the using the same solutions for
maintenance1. Mild tissue inflammation
can occur in the anterior segment of
the eye, not severe enough to cause
red or sore eyes, but enough to create
discomfort and symptoms such as
burning, itching, "aching" eye, "hot" or
dry eye sensation, foreign body or
"sand in the eyes" sensations, etc.
In many cases, these understated
symptoms have no obvious clinical
signs but can cause great discomfort
accompanied by, if not caused by,
a collapse of the pre-corneal film
structure and can be generically
defined as "marginal dry eye".
In our study, we paid particular
attention to the Ferning Test results
portatori di LAC hanno dichiarato che le
due ragioni principali per le quali hanno
smesso di portare le lenti a contatto sono la
secchezza oculare e il fastidio oculare nella
parte finale della giornata17.
Il discomfort in realtà dovrebbe essere
visto anche come problema multifattoriale,
dato che può essere determinato da una
vasta gamma di fattori a partire da quello
ottico correttivo, per andare poi a quelli
concernenti la fisiologia e la biochimica
dell’occhio. Consideriamo ad esempio
l’aspetto rifrattivo e ricordiamoci come
spesso il comfort delle lenti sia influenzato in
modo consistente dalla giusta correzione.
Altri fattori importanti possono essere dati
dalla ridotta ossigenazione, dalla formazione
di depositi, dall’azione meccanica della lente,
dalla cattiva pulizia delle lenti o dalle stesse
soluzioni utilizzate per la manutenzione1.
Si possono creare ad esempio lievi
infiammazioni o sensibilizzazioni a livello dei
tessuti del segmento anteriore dell’occhio,
non forti abbastanza da rendere l’occhio
rosso o dolorante ma sufficienti a dare
discomfort e sintomi come bruciori, pruriti,
occhio “indolenzito”, sensazione di occhio
“caldo” o asciutto, sensazioni di corpo
estraneo o “sabbia negli occhi”, ecc.
In molti casi questa sintomatologia sottile,
senza segni clinici evidenti ma fortemente
disturbante, è accompagnata se non
provocata, da un collasso nella struttura
del film pre corneale e può essere definita
216
Usefulness of trehalose for contact lens wearers
as various authors have pointed to
its usefulness as a predictive test
to gauge the risk of intolerance
in patients who are candidates
for contact lenses10-11. It is welldocumented that patients with a high
Ferning rating (ie. Type IV) are at high
risk of intolerance to contact lenses.
In such cases, the identification of risk
offers the opportunity to customise
contact lens’ selection and instructions
for use. Although the mechanisms and
biochemical processes of the ferning
are still not completely clarified, it is
commonly agreed that the ferning
process results from interaction
between electrolytes (Na+ Cl- and K+
Cl-) and globular material consisting
of glycoproteins with high molecular
weight of the mucus (mucin). The
mucus component coats the salt
molecules affecting the shape of
the ferns. In the absence of protein
or in the presence of an excessive
amount of salts (eg. in eyes with hyper
evaporation), new salt molecules are
deposited around the central nucleus
of the ferns, preventing branching. In
the presence, however, of abundant
glycoprotein material, this material
is deposited at the front apex of the
crystallisation preventing its advance
and forcing it to branch and form the
ferns.
The results of this study suggest
that trehalose can be useful in the
reinstatement of all the tear film layers,
creating a valid alternative for those not
benefitting from other tear substitutes.
In fact, a simultaneous and significant
improvement of all subjective and
objective parameters under analysis
was observed. These results acquire
an even more significant clinical value
when the type of patients studied is
considered: wearers of RGP lenses for
advanced keratoconus with overt CLD
genericamente come condizione di “occhio
secco marginale”.
Nel nostro studio abbiamo dedicato
particolare attenzione ai risultati del test
di felcizzazione in quanto vari autori
ne hanno suggerito l’utilità come test
predittivo del rischio di intolleranza
nei pazienti candidati all’uso di lenti
a contatto10-11. È infatti noto che i
pazienti con un test di felcizzazione di
punteggio elevato (es. tipo IV) sono ad
elevato rischio di intolleranza alle LAC,
e l’identificazione del rischio offre al
prescrittore l’opportunità di personalizzare
la scelta della LAC e delle modalità di
uso. Anche se i meccanismi ed i processi
biochimici della felcizzazione sono tuttora
non completamente chiarificati, si ritiene
che il processo di felcizzazione derivi dalla
interazione tra elettroliti (Na+Cl- e K+Cl-)
e materiale globulare costituito da
glicoproteine ad alto peso molecolare del
muco (mucine). La componente mucinica
riveste le molecole di sale condizionando
la forma delle felci. In assenza di
proteine o in presenza di una quantità
eccessiva di sali (es. negli occhi con iper
evaporazione) nuove molecole di sale
si depositano intorno al nucleo centrale
delle felci, impedendone la ramificazione.
In presenza, invece, di abbondante
materiale glicoproteico, questo si deposita
all’apice del fronte di cristallizzazione
impedendone l’avanzamento e
costringendo il sistema a ramificarsi e a
formare le felci.
I risultati osservati in questo studio
suggeriscono che il trealosio possa
essere utile al reintegro di tutti gli strati
del film lacrimale così da consentire
una valida alternativa a tutti coloro che
con altri sostituti lacrimali non trovano
giovamento. Infatti abbiamo osservato
un contemporaneo e significativo
miglioramento di tutti i parametri
soggettivi ed oggettivi analizzati.
Tali risultati acquisiscono una valenza
Year 1 ı Number 4 ı 2015
217
Utilità di trealosio nei portatori di lenti a contatto
and at high risk of discontinuing use.
TTrehalose effectiveness in these
subjects makes it a highly interesting
option, not only in terms of CLD and
tear evaporation treatment of CLD,
but also in terms of prevention for
those patients who, at initial evaluation
prior to wearing contact lenses,
already showed signs of risk factors
for tear evaporation. In conclusion, it
is our opinion that trehalose 3% tear
substitute can permit patients to wear
RGP lenses even when they are at
high risk of intolerance and whose only
other alternative is to wear glasses.
In cases of advanced keratoconus,
glasses do not guarantee sufficient
visual acuity. Positive impacts on the
patient with keratoconus’ quality of life
and improved quality of vision have to
both be taken into consideration.
ABSTRACT
Contact lens discomfort (CLD) is
considered the leading cause of
discontinuation of contact lens use,
regardless of type and reason for
use. Those using rigid gas permeable
lenses (RGP lenses) for advanced
keratoconus can be considered at a
high risk of CLD.
Objective: To evaluate the
effectiveness of trehalose 3% eye
drops in relieving ocular discomfort
and improving quality and quantity
of tear film in patients with advanced
keratoconus and Rigid gas permeable
lenses (RGP lenses) wearers showing
signs of CLD despite regular
administration of a tear substitute. The
study enrolled 31 patients who had
been wearing rigid gas permeable
lenses (RGP lenses) for advanced
keratoconus for more than 3 months
and who showed CLD and tear
evaporation, defined through alteration
in at least two tear film function tests
clinica rilevante anche in funzione
della tipologia dei pazienti, portatori di
LAC-RGP per cheratocono avanzato
con CLD conclamato ad elevato rischio
di abbandono. L’efficacia di trealosio in
questi soggetti lo rende un candidato
di sicuro interesse non solo in un’ottica
di trattamento di CLD e dislacrimia,
ma anche nella sua prevenzione in
tutti i pazienti che alla valutazione
effettuata prima di applicare una lente a
contatto già presentino fattori di rischio
di dislacrima. In ultima analisi quindi il
sostituto lacrimale a base di trealosio 3%
consente a nostro avviso di applicare
LAC-RGP anche in pazienti ad elevato
rischio di intolleranza che in alternativa
hanno solo la possibilità di usare gli
occhiali. Che notoriamente nei casi di
cheratocono avanzato non garantiscono
un visus sufficiente. Inutile sottolineare
anche l’impatto sulla qualità di vita dei
pazienti affetti da cheratocono oltre a
quello sulla qualità della visione.
RIASSUNTO
Il discomfort da lente a contatto (CLD)
viene ritenuto la principale causa di
abbandono delle lenti a contatto (LAC),
indipendentemente dal tipo e motivo
di utilizzo. I portatori di lente rigida gas
permeabile (LAC-RGP) per cheratocono
avanzato possono essere considerati ad
alto rischio di CLD.
Scopo dello studio: valutare l’efficacia
di un collirio a base di trealosio 3%
nell’alleviare il discomfort oculare
e migliorare qualità e quantità del
film lacrimale in pazienti affetti da
cheratocono avanzato e portatori di
lente rigida gas permeabile (LACRGP) con evidenza di CLD malgrado
la somministrazione regolare di un
sostituto lacrimale. Sono stati arruolati
31 pazienti portatori da oltre 3
mesi di LAC-RGP per cheratocono
avanzato che presentavano CLD e
218
Usefulness of trehalose for contact lens wearers
(B.U.T., Schirmer Test and Ferning Test)
associated with insufficient maximum
time permitted for the use of contact
lenses/day (<4 hours). A change in
tear substitute was proposed before
carrying out further evaluation.
Schirmer, Break Up Time (B.U.T.) and
Ferning Tests were performed during
the selection (baseline) process. In
addition, patients were surveyed on
maximum number of hours/day that
contact lenses were worn for the
3 days prior to the visit, and their
overall degree of satisfaction with
wearing contact lenses (score 0-5). All
selected patients were already being
treated with a carboxymethylcellulose
based tear substitute (4 instillations/
day) which was replaced by trehalose
3% eye drops (4 instillations/day)
after the initial visit. At the 8-week
(final) check-up following the switch
to trehalose 3%, all patients showed
a marked improvement in signs of
CLD and quantitative parameters of
tear film (B.U.T. medium increase from
7 seconds to 13, medium increase
in Schirmer Test from 10 to 15 mm,
improvement in Ferning Tests from
Type III or IV at the baseline visit to
Type I or II at the final one), and a
significant increase in the maximum
contact lens wearing time, from an
average 3.5 hours/day to 8 hours/
day. Moreover, patient satisfaction
levels regarding contact lens wearing
increased from a medium baseline
value of 0.5 to 4.5 at the final visit.
Conclusions: In users of rigid gas
permeable lenses (RGP lenses) for
advanced keratoconus with obvious
signs of intolerance and at risk of
discontinuing use, the switch to
trehalose 3% eye drops alleviated both
CLD and tear evaporation to a clinically
significant level. Regular application
of trehalose eye drops can offer an
dislacrimia, definiti dall'alterazione di
almeno due test di funzionalità del film
lacrimale (B.U.T., test di Schirmer e
test di felcizzazione) dall'alterazione di
cambiare il sostituto lacrimale, prima
di valutare ulteriori provvedimenti. In
occasione della visita di selezione
(basale) sono stati effettuati test di
Schirmer, Break up time (B.U.T.), test
di felcizzazione, rilevazione del numero
massimo di ore/die di utilizzo LAC nei
3 giorni precedenti la visita, giudizio
globale del paziente sul grado di
soddisfazione nell’indossare le lenti a
contatto (scala verbale da 0 a 5). Tutti
i pazienti selezionati già utilizzavano
un sostituto lacrimale a base di
carbossimetilcellulosa (4 istillazioni/die)
che a decorrere da tale visita è stato
rimpiazzato da un collirio a base di
trealosio 3% (4 istillazioni/die).
Alla visita di controllo (finale) 8
settimane dopo lo switch a trealosio
3%, si è osservato in tutti i pazienti un
netto miglioramento dei segni di CLD
e dei parametri quali-quantitativi del
film lacrimale (incremento del B.U.T.
medio da 7 secondi a 13 secondi,
incremento test di Schirmer medio da
10 a 15 mm, miglioramento del test di
felcizzazione da tipo III o IV della visita
basale a tipo I o II di quella finale) ed
un significativo incremento del tempo
massimo di utilizzo LAC, passato da
una media di 3,5 ore/die ad 8 ore/die.
Anche il giudizio globale sul grado di
soddisfazione del paziente nell’indossare
LAC è aumentato da un valore medio
basale di 0,5 a 4,5 alla visita finale.
Conclusioni: nei portatori di lente
rigida gas permeabile (LAC-RGP) per
cheratocono avanzato con evidenti
segni di intolleranza ed a rischio di
abbandono, lo switch ad un collirio
a base di trealosio 3% ha consentito
di alleviare in maniera clinicamente
rilevante CLD e dislacrimia.
Year 1 ı Number 4 ı 2015
219
Utilità di trealosio nei portatori di lenti a contatto
alternative treatment option in cases
of CLD due to RGP lenses, prior to
considering alternate action.
La regolare applicazione di un collirio
a base di trealosio può rappresentare
un’alternativa terapeutica nei casi di
CLD da LAC-RGP, prima di considerare
ulteriori provvedimenti.
REFERENCES
1)
2)
3)
4)
5)
6)
7)
8)
9)
10)
11)
12)
13)
Nichols JJ, et al. The TFOS International
Workshop on Contact Lens Discomfort:
executive summary. Invest Ophthalmol Vis Sci
2013;54:7-13
Young G, Veys J, Pritchard N, Coleman S.
A multi-centre study of lapsed contact lens
wearers. Ophthalmic Physiol Opt 2002;22:51627
Holly FJ, Lemp MA. Wettability and wetting of
the corneal epithelium. Eye Exp Res 1971;11:
239-51
Barnett M, Mannis MJ. Contact lenses in
the management of keratoconus. Cornea
2011;30:1510-16
Franklin A, Franklin N. Rigid Gas-permeable
Lens Fitting. UK: Butterworth-Heinemann,
Elsevier; 2007. p. 106-16
Dogru M, et al. Tear function and
ocular surface changes in keratoconus.
Ophthalmology 2003;110:1110-18
Fath-Elrahman N, et al. The effects of rigid
gas-permeable contact lens wear on tear film
of eyes with keratoconus. Sudanese Journal of
Ophthalmology 2015;7:6-9
Moon JW, et al. The effect of contact lens wear
on the ocular surface changes in keratoconus.
Eye Contact Lens 2006;32:96-101
Zhou AJ, et al. Contact lens care in
keratoconus. Cont Lens Anterior Eye
2003;26:171-74
Kogbe O, Liotet S. An interesting use of the
study of tear ferning patterns in contactology.
Ophthalmologica 1987;194:150-53
Ravazzoni, et al. Forecasting of hydrophilic
contact lens tolerance by means of tear
ferning test. Graefes Arch Clin Exp Ophthalmol
1998;236:354-58
The TFOS International Workshop on Contact
Lens Discomfort. Report of the Management
and Therapy Subcommittee. Invest Ophthalmol
Vis Sci 2013;54:183-203
Ramamoorthy P, Sinnott LT, Nichols JJ.
Treatment, material care, and patient-related
factors in contact lens-related dry eye. Optom
Vis Sci 2008;85:764-72
14) Begley CG, Chalmers RL, Mitchell GL, et al.
Characterization of ocular surface symptoms
from optometric practices in North America.
Cornea. 2001;20:610-18
15) Luyks J , Baudouin C. Trehalose: an intriguing
disaccharide with potential for medical
application in ophthalmology. Clinical
Ophthalmology 2011:5 577-81
16) Rolando M. Tear mucus ferning test in normal
and keratoconjunctivitis sicca eyes. Chibret Int
J Ophthalmol 1984;2:33-41
17) Begley C, et al. Characterization of Ocular
Surface Symptoms From Optometric Practices
in North America. Cornea 2001;20:610-18