Artrite reumatoide oggi:
cosa è importante sapere
per il MMG
M Matucci Cerinic
SOD Reumatologia AOUC
Università di Firenze
Cosa è importante sapere per il MMG ?
1.
2.
3.
4.
La diagnosi precoce è possibile
Comorbidità
Effetti collaterali dei farmaci
Conclusione
La diagnosi precoce è possibile oggi
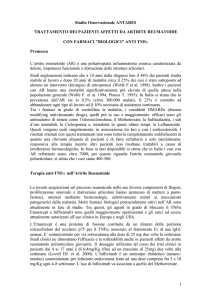
Course of Rheumatoid Arthritis:
Schematic Representation
Severity
(arbitrary units)
Inflammation
Disability
Radiographs
0
5
10
15
20
Duration of disease (years)
Kirwan JR. J Rheumatol. 1999;26:720-725.
25
30
DANNO ARTICOLARE NELLA ARTRITE
REUMATOIDE E’ PRECOCE
EROSIONI OSSEE NEL 75% DEI
PAZIENTI CON
ARTRITE REUMATOIDE PRECOCE
Arthritis Rheum. 2002 feb.
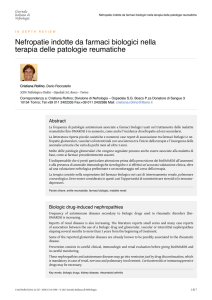
Artrite Reumatoide, inabilità al lavoro…
% abilità al lavoro
Anni di malattia
I problemi del lavoro nella AR
Il 10% dei pazienti con AR smette di lavorare
entro 1 anno dalla diagnosi
Il 50% smette di lavorare entro 10 anni dalla
diagnosi
Il 60% smette di lavorare entro 15 anni dalla
diagnosi
Il 90% abbandona il lavoro entro 30 anni dalla
diagnosi
Yelin E et al, Arthritis Rheum 30:507–512, 1987
RHEUMATOID ARTHRITIS
Economic Burden (Europe)
– In West Germany, the costs of RA were >40 billion DM
(US $17.6 billion) in 1994 for treatment alone
– In the UK, average RA outpatient cost/case/year was £798
(US $1,126) and £1,253 (US $1,769) per inpatient in 1997
– RA per capita costs average:
•
•
•
•
49% of cost of cancer
68% of cost of stroke
82% of cost of coronary heart disease
5X cost of motor vehicle accidents
Knorr U. Versicherungsmedizin. 1994.
Rothfuss J. Akt Rheumatol. 1997.
Lubeck DP et al. Arthritis Rheum. 1986;29:488–493.
Lorig KR et al. Arthritis Rheum. 1993;36:439–446.
Costi dell’AR
• Diretti: 380 mil Euro
Spese ricoveri, farmaci, acertamenti diagnostici,
visite (a carico paz e SSN)
• Indiretti: 1210 mil Euro
spese sostenute dalla collettività, mancati guadagni
dovuti a invalidità
Costi Complessivi 1600 mil Euro
Costi Ombra: a carico del malato e suoi familiari per
far fronte alla malattia
Difficilmente quantizzabili, si aggirano all’incirca
attorno ad un MILIARDO di Euro
Obiettivi del trattamento dell’AR
Alleviare i sintomi
Conservare la funzionalità
Prevenire il danno strutturale e le deformità
Mantenere o recuperare il normale stile di
vita del paziente
Sicurezza a lungo termine
Akil M, Amos RS, BMJ 310:587–590, 1995
AR Precoce
il medico di medicina generale od
altro specialista deve sospettare
una artrite in fase precoce ed inviare
il paziente al reumatologo quando
osserva;
1. 3
2.
articolazioni tumefatte
Coinvolgimento delle MTF/MCFtest della gronda positivo
3. Rigidità
mattutina 30 minuti
DANNO ARTICOLARE NELLA
ARTRITE REUMATOIDE E’
PRECOCE
• Il danno inizia entro i primi tre mesi
• Entro i primi tre mesi è necessaria la diagnosi
STRATEGIA TERAPEUTICA
ATTUALE
TRATTAMENTO
AGGRESSIVO NELLE
PRIME FASI ( primi 3 mesi )
E’ oggi possibile ottenere una diagnosi più
precoce di AR con l’aiuto di parametri clinici
di laboratorio, genetici, e di diagnostica per
immagini di vario tipo che abbiano un valore
predittivo.
…dobbiamo evitare che l’ansia di una ricerca
di diagnosi molto precoce vada a scapito di
un corretto inquadramento diagnostico e di
un corretto approccio terapeutico…
(S. Bombardieri - SIR 2006)
Dogmi…
1. La diagnosi deve essere formulata nella fase precoce
dell’AR entro i primi 3 mesi di malattia
2. La diagnosi deve essere formulata e la terapia iniziata prima
che abbia inizio le erosioni che danneggino in maniera
irreversibile le articolazioni e la loro funzione.
Management of patients with RA, Therapeutic
Sustained Remission
Prevention /
reversal of
disability
objectives
Prevention / arrest
of joint damage
Prevention of systemic co-morbidities:
CV diseases, osteoporosis….
Comorbidità
Comorbidities in rheumatoid arthritis
Glaucoma
Depression
Renal
disease
Osteoporosis
Comorbidità
Cataract
Infection
Anemia
Malignancy
Gastrointestinal
disease
Pancreatitis
Easy bruising
Diabetes
Lung
involvement
Neurological
manifestations
Cardiovascular
disease
Cardiovascular risk factors in rheumatoid arthritis (RA)
Traditional risk
factors
Age
BMI
Dyslipidemia
Hypertension
Diabetes mellitus
Smoking
Family hystory
Sedentary life style
Homocysteine
Insulin-resistance
RA-related risk factors
Inflammation-mediated
Adhesion molecules (VCAM-1 / ICAM-1)
Proinflammatory cytokines (TNF-α, IL-1, IL-6)
C-reactive protein
MCP-1
Immune-mediated
Rheumatoid factor
Anti-CCP
ACL
anti-oxLDL
CD4+CD28null T cells
Oxidative stress (oxLDL, proinflamm. HDL)
Endothelial progenitor cells (EPC)
TREATMENT
LIPID
PROFILE
DISEASE
ACTIVITY
Inflammation
Autoimmunity
Jick, ARD 2009;68:546
Choy, ARD 2009;68:460
Gerli, Arthritis Care Res 2010;62:712
Myasoedova, ARD 2011;70:482
Bartels, Arthritis Rheum 2011;63:1221
HDL
Rheumatoid arthritis
Apo-AI
Apo-B
Apo-B / ApoAI
ratio
INFLAMMATION AND LIPID INTERACTION
IN RHEUMATOID ARTHRITIS
Inflammation
degree
Complexity of lipid
evaluation
Drug effects
Hydroxychloroquine Use Associated With Improvement in Lipid
Profiles in Rheumatoid Arthritis Patients
LDL (mg/dl)
LDL/HDL
HDL (mg /dl)
Chol/HDL
Total cholesterol (mg/dl)
Triglycerides (mg/dl)
Morris S et al. Arthritis Care Res 2011;4:530-4
Anti-RA drugs decrease CV risk
• Case control study
• 72 with history of CV
events; 541 without history
of CV events
• All patients anti-TNF-naïve
• Analysis: Corrections for age,
gender, smoking, RA
duration
HTN, DM,
0,35
0,3
0,25
0,2
0,15
0,16
0,16
0,11
0,1
0,05
,elevated cholesterol,
0
RF status, and erosions
van Halm VP,et al. ACR
0,37
0,4
Risk for CV Event
MTX only
SSZ only
MTX+SSZ
Triple
Effects of DMARDs on lipid levels in rheumatoid arthritis
42 RA patients
treated with DMARDS (essentially MTX) for 12 months
HDL cholesterol by 21% (p<0.001)
apolipoprotein A-I by 23% (p<0.001)
LDL/HDL cholesterol ratio (N.S.)
Significant differences between responders and nonresponders in
the mean 12-month changes in:
HDL cholesterol
apolipoprotein A-I
LDL/HDL cholesterol ratio
Park Y-B et al. Am J Med 2002;113:188-93
Effect of TNF inhibitors on lipid profile in RA:
a systematic review with meta-analysis
Daien CI et al. Ann Rheum Dis 2012;71:862-8
DYSLIPIDAEMIA INDUCED BY INFLAMMATION
IL-6
TNF-α
LIVER
CRP
Total cholesterol
HDL
Triglycerides
Small dense LDL
ApoB/ApoAI
DYSLIPIDAEMIA INDUCED BY INFLAMMATION
IL-6
TNF-α
LIVER
Treatment
effect
Total
Totalcholesterol
cholesterol
HDL
HDL
Triglycerides
Triglycerides
Small
Smalldense
denseLDL
LDL
ApoB/ApoAI
ApoB/ApoAI
CRP
Effetti collaterali della terapia
Risk factors of serious adverse events in RA
Risk factors of serious Infections
Age (≥ 60,≥≥ 80)
Previous serious infection (in the past year +)
Corticosteroid use (dosage )
Elevated ESR
Systemic manifestations
Comorbidities (Coronary Heart Disease,Heart failure,peripheral vascular disease,chronic lung
disease, diabetes, alcoholism)
Biologics ?
Crowson S et al Arthritis Rheum 2012;64: 2847-55. Curtis JR et al. Arthritis Rheum. 2007;56:112; Srangfeld A et al Ann Rhem Dise 2012;70 :1914-20
Predictors and Risk of Infection in
Rheumatoid Arthritis
Relative Risk to general population: 1.9 [1.7 – 2.1]
Best predictors:
RA severity / disease activity
Age
Corticosteroid therapy
Comorbid diseases: CVD, CHF, CRF, DM, lung disease
Previous infection
Joint surgery
Contributory role of DMARDs not clearly defined
Moreland et al. J Rheum 2001;28:1238-44.
Safety of biologics in patients with RA
Serious infections:
Rate from 2 to 8 / 100 patient-Years depending of the studies (RCTs vs registries),
and patients populations
Opportunistic infections including TB:
Reported for all biologics
Tb screening recommended for all biologics but RTX
Malignancies and lymphomas:
No signal
Injection reactions
Others: Transaminases, lipides, neutropenia
Dixon W, et al. Arthritis Rheum 2006;54:2368-76; Weinblatt M et al Arthritis Rheum 2006;54:2807-16;Gottenberg J et al Arthritis Rheum. 2010 ;58: Mariette
et al, Ann Rheum Dis. 2011;70:1895-904 ;Smolen J et al Ann Rheum dis 201o
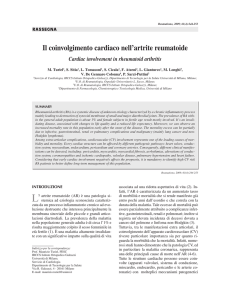
Cancers risk in RA Patients
RA cohort (n=66 471) - 0.7% of Swedish population alive in
1998, identified in 3 overlapping national registers
Followed through to 2005
Cancer in RA not treated with anti-TNF
Relative risk of cancer
All site, 3742
Respiratory tract, 410
Upper GI, liver, pancreas, 300
Colorectal, 329
Breast, 534
Ovary, Uterus, Cervix, 227
Prostate, Testes, 530
Kidney, Bladder, 253
Skin, melanoma, 115
Skin, non-melanoma, 306
Central nervous system, 72
Other, 279
1.11 (1.08, 1.16)
1.35 (1.21, 1.51)
1.12 (0.98, 1.27)
0.75 (0.67, 0.85)
0.94 (0.86, 1.03)
0.83 (0.72, 0.96)
1.06 (0.96, 1.16)
1.22 (1.06, 1.41)
1.14 (0.93, 1.40)
1.76 (1.54, 2.01)
1.09 (0.84, 1.41)
1.29 (1.12, 1.47)
0
1
2
3
4
Askling J, et al EULAR 2007, Barcelona, #OP0013
Increased risk of lymphoma in RA Swedish matched case control study
Cases
no.(%)
Controls
no.(%)
Unadjusted OR
no.(%)*
Low
94 (25)
278 (74)
1 (referent)
Medium
196 (52)
94 (25)
7.7 (4.8-12.3)
High
86 (23)
4 (1)
71.3 (24.1-211.4)
I
34 (9)
138 (37)
1 (referent)
II
185 (49)
204 (54)
3.9 (2.4-6.3)
III
105 (28)
31 (8)
13.8 (7.2-26.2)
IV
52 (14)
3 (1)
67.5 (18.9-239.8)
Inflammatory activity†
Functional class‡
† Score reflecting the entire period from onset
of rheumatoid arthritis (RA) until diagnosis of
lymphoma, based on TJC, SJC, ESR, and PGA
‡ Steinbrocker criteria 1 year before lymphoma
diagnosis
Risk of lymphoma is substantially increased in a subset of patients with RA, those
with very severe disease
High inflammatory activity, rather than its treatment, is a major risk determinant
376 patients with RA complicated by malignant lymphoma and 376 matched controls
Baeklund E, et al. Arthritis Rheum 2006;54:692-701
Conclusioni
1.Diagnosi precoce
2.Valutazione delle comorbidità
3.Bilanciamento terapia
4.Attenzione alle infezioni
5.Attenzione alla possibile evoluzione neoplastica