Le resistenze di HIV
sono destinate a scomparire?
Andrea De Luca
Istituto di Clinica delle Malattie Infettive
Univ. Cattolica S. Cuore, Roma
Malattie Infettive Universitarie, AOU, Siena
Background
• I trattamenti più potenti e ad elevata barriera
genetica dovrebbero determinare una riduzione
delle resistenze
• Sempre meno pazienti in trattamento presentano
viremie rilevabili
• Se la fonte primaria delle resistenze (i pazienti in
fallimento con resistenze) viene ad esaurirsi, le
resistenze dovrebbero scemare
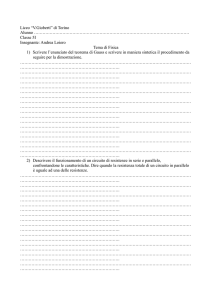
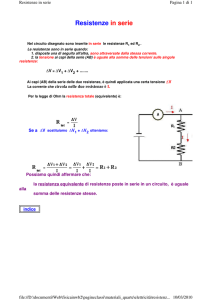
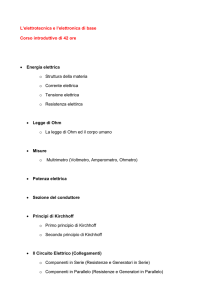
Prevalence of HIV resistance at several classes: all
ARV-treated individuals (ARCA db; n=4,887)
100
90
80
percent of patients
70
Resistance NRTI
60
Resistance NNRTI
50
Resistance PI
40
Resistance any class
Multidrug resistance
30
Non B subtypes
20
10
0
1999 2000 2001 2002 2003 2004 2005 2006
n= 395
362
490
488
760
974
829
224
Di Giambenedetto et al. Antivir Ther 2009
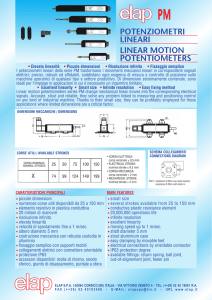
100
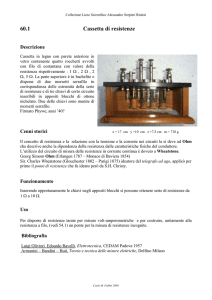
Prevalence of HIV resistance at several classes:
in first line cART failures (ARCA db; n=717)
90
percent of patients
80
70
60
Resistance NRTI
50
Resistance NNRTI
Resistance PI
40
Resistance any class
30
Multidrug resistance
20
Non B subtypes
10
0
1999
n= 52
2000
2001
2002
2003
2004
2005
2006
52
64
68
126
163
116
26
Di Giambenedetto et al. Antivir Ther 2009
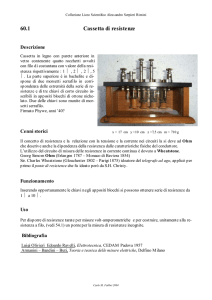
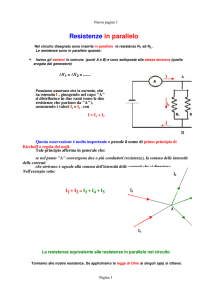
Surveillance of the Epidemiology of Emergent
HIV drug Resistance in Europe (SEHERE) (n=20763)
Di Giambenedetto S et al. EACS 2009
Resistance to Drug Classes per Calendar Year
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
NRTI
n= 365
839
1620
2027
2199
NNRTI
2306
PI_major
2591 2731 2581 1900 1274
325
Di Giambenedetto S et al. EACS 2009
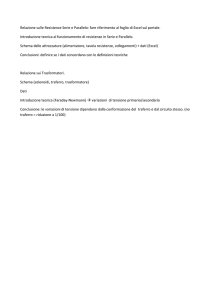
Prevalence of different non-B subtypes
by calendar year
12
02_AG
14_BG
29_BF
A1
C
D
G
Other
10
%
8
6
4
2
0
199719981999200020012002200320042005200620072008
Di Giambenedetto S et al. EACS 2009
Di Giambenedetto S et al. EACS 2009
Prevalence of type 1 TAMs
over calendar years
Di Giambenedetto S et al. EACS 2009
Prevalence of other NRTI-RM
over calendar years
Di Giambenedetto S et al. EACS 2009
Prevalence of NNRTI-RM
over calendar years
Di Giambenedetto S et al. EACS 2009
Prevalence of selected major PI-RM
over calendar years
Di Giambenedetto S et al. EACS 2009
Di Giambenedetto S et al. CROI 2010
Prevalence of transmitted
HIV-1 drug resistance in Italy (n=1690)
Bracciale L J Antimicrob Chemother 2009
Prevalence of transmitted HIV-1 drug
resistance in Italy: subtype B only
Bracciale L J Antimicrob Chemother 2009
Decline in transmitted HIV-1 drug resistance in the UK
All patients
(n = 4454)
Acutely infected
(n = 316)
NRTI
NNRTI
PI
UK Collaborative Group on HIV Drug Resistance, AIDS 2007
Resistance can be transmitted from one
individual to another
• Drug resistant virus is prevalent in primary infection
and the transmission of resistant virus from
individuals who have failed antiretroviral therapy is
well
documented
– Reviewed by Tang JW & Pillay D. J Clin Virol 2004; 30:1–10
• Transmitted resistant virus persists for long periods
of time
–
–
–
Pao D, et al. JAIDS 2004; 37:1570–1573
Little S, et al. Antirvir Ther 2003; 8:S129
Brenner B et al. AIDS. 2004; 18:1653–1660
• Resistant virus can be ‘re-transmitted’ from one
treatment-naive individual to another
–
–
Taylor S et al. AIDS Res & Hum Retroviruses 2003; 19:353–361
DeMendoza et al. Clin Inf Dis 2005; 41;1350–1354
‘Transmission chains’ could generate an undetected epidemic of infection
with drug resistant virus
How much does transmitted DR
depend from emerging DR?
Probabilità di trasmissione di DR:
-efficienza intrinseca
-carica virale
-frequenza e modalità di
esposizione
EDR
EDR
TDR
TDR
Probabilità di trasmissione di DR:
>per mutazioni ad alta fitness
>da pazienti off-therapy
>in pazienti a diagnosi ignota
>a pazienti non in terapia
TDR
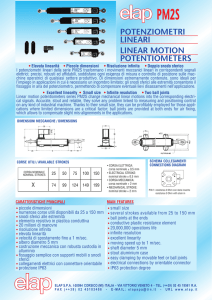
Analisi filogenetica in pazienti naive (ARCA,
prima sequenza, sottotipo B, n=442)
10
9
Percent resistant
8
7
6
any R
5
NRTI R
4
NNRTI R
maj PI R
3
2
1
0
resistance class
Assessment dei cluster
tramite analisi filogenetica bayesiana
Branch lengths expressed in
nt substitutions per site
Analisi filogenetica in pazienti naive (ARCA,
prima sequenza, sottotipo B, n=442)
• ML con 100 bootstrap runs:
– 44 cluster identificati (mediana 2 pazienti: range 2-7)
– 112/442 sequenze (25.3%) in cluster di naive
– 7/44 cluster (15.9%) contengono resistenze
– 13/41 (31.7%) sequenze con resistenze sono in cluster
– 99/401 (24.7%) sequenze senza resistenze sono in
cluster
Cluster con sequenze discordanti
riguardo le resistenze
• 7 cluster con resistenze:
– 3 concordanti (tutte le sequenze con
resistenze)
– 4 discordanti (alcune sequenze con
resistenze, altre senza)
Potenziali cause di discordanza
rispetto alle resistenze nei cluster
Trattamento e fallimento
Paziente 1
noR
Paziente 2
EDR
TDR
Potenziali cause di discordanza
rispetto alle resistenze nei cluster
Paziente 1
noR
Paziente 2
-Resistenze non rilevabili
(quasispecie minoritarie)
TDR
-Resistenze non
trasmesse (minore fitness
virale, bottleneck)
Studi futuri per comprendere il
fenomeno dei cluster discordanti
• Ampliamento del campione
• Dinamica temporale?
• Studio della direzionalità delle trasmissioni
• Necessità di studio di sequenze longitudinali
De Luca A Curr Op HIV AIDS 2009, in press
Conclusions:
is HIV drug resistance disappearing?
• Improved treatments and more active new
agents are reducing EDR
• There are reports of reduced TDR
• Nonetheless, TDR is continuously fuelled by
treatment naive individuals with at risk
behaviors
• The entity of TDR derived from treated and
from naive patients requires clarification
Conclusions:
is HIV drug resistance disappearing?
• Interventions towards naive individuals:
– Earlier diagnosis
– Behavioral changes
– Treatment
may significantly reduce TDR
• In the future there might be a further reduction of EDR and
TDR, but DR disappearance probably a dream:
– EDR and TDR in low-middle income countries
– Durability of current regimens
• Will depend on wise and rationale
usage/sequencing
• No big news at the horizon
Acknowledgements
Acknowledgements
•
•
•
•
•
•
•
D Dunn, D Pillay, C Sabin UK-HIVDR and CHIC
R Camacho, Lisbon
M Ciccozzi, A Lo Presti, ISS, Roma, Italy
P Sloot, Univ. of Amsterdam, the Netherlands
ARCA: M Zazzi, C Balotta
Euresist: ARCA, AREVIR (R Kaiser), Karolinska (A. Sonnerborg)
Virolab: FP6 INFSO-IST-027446 (C Torti, D vd Vjver, AM
Vandamme)
• Computing Real-World Phenomena with Dynamically
Changing Complex Networks (DYNANETS): FP7-233847
• Collaborative HIV and Anti-HIV Drug Resistance Network
(CHAIN): FP7 HEALTH-2007-B -223131
Special acknowledgements
Iuri Fanti, B.Eng.CS
Mattia Prosperi, PhD