ULTRASONOGRAPHIC IMAGING OF BICEPS TENDON RUPTURE
AT THE MYOTENDINOUS JUNCTION.
ENGLISH
Rafailidis V 1, Delianidou A 2, Sferopoulos N2, Torounidis
I2
1. Radiology Department, AHEPA University Hospital,
Thessaloniki, Greece.
L’IMAGING ECOGRAFICO DELLA ROTTURA DEL TENDINE DEL
BICIPITE ALLA GIUNZIONE MIOTENDINEA
ITALIAN TRANSLATION
Rafailidis V 1, Delianidou A 2, Sferopoulos N2, Torounidis
I2.
1. Radiology Department, AHEPA University Hospital,
Thessaloniki, Greece.
2. Radiology Department, “G. Gennimatas” General
Hospital of Thessaloniki, Thessaloniki, Greece.
2. Radiology Department, “G. Gennimatas” General
Hospital of Thessaloniki, Thessaloniki, Greece.
Corresponding author: Vasileios Rafailidis, Radiology
Department, AHEPA University Hospital, Thessaloniki,
Greece; Email: [email protected]
Corresponding author: Vasileios Rafailidis, Radiology
Department, AHEPA University Hospital, Thessaloniki,
Greece; Email: [email protected]
Case Description
A 57-year-old male patient presented complaining of
decreased strength of his arm during flexion and supination
along with a soft tissue lump in the anterior aspect of the
distal arm. The patient described hearing a “popping”
sound in his arm while trying to elevate something heavy,
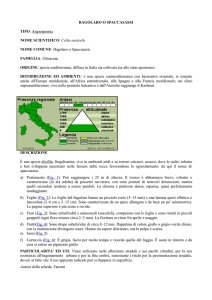
ten days ago. Clinical examination revealed the “popeye’s”
sign in the affected arm (Fig. 1).
An ultrasound examination using a 5-13 MHZ linear
transducer with scan width 37 mm was performed
including grayscale, colour Doppler and eFlow imaging.
Extended field of view imaging was used to evaluate the
whole length of the muscle belly and tendon during
contraction and relaxation. There was a fluid filled focal
defect at the myotendinous junction, while the tendon
appeared normal inside the groove. The belly of the long
head was retracted and surrounded by fluid, but retained
its normal echotexture (Fig. 2-6).
Follow-up examination one month later revealed the defect
at the myotendinous junction and hyperemia of the muscle
and tendon ends. The long head biceps belly appeared
more echogenic compared to the short head of the biceps
belly, producing the “white and black appearance” (Fig. 78).
Descrizione del caso: un uomo di 57 anni si presentava alla
nostra attenzione lamentando una riduzione della forza del
braccio durante la flessione e la supinazione associata ad
una bozzatura dei tessuti molli della porzione anteriore e
distale del braccio stesso. Il Paziente descriveva di aver
udito un rumore secco mentre cercava di sollevare
qualcosa di pesante circa 10 giorni prima. La valutazione
clinica dimostrava il segno di “braccio di ferro” a livello del
braccio interessato (Fig. 1).
L’esame ecografico condotto utilizzando una sonda lineare
da 5-13 MHz con un’ampiezza di scansione di 37 mm
includeva l’ecografia in scala di grigi, il color-Doppler e
l’imaging eFlow. Il campo di vista esteso è stato usato per
valutare l’intera lunghezza del ventre muscolare e del
tendine durante la contrazione e il rilassamento.
All’ecografia era evidente un difetto focale alla giunzione
miotendinea riempito di fluido mentre il tendine appariva
normale entro la doccia. Il ventre muscolare del capo lungo
era retratto e circondato da fluido ma presentava
un’ecostruttura normale (Fig. 2-6).
L’esame di follow-up un mese dopo mostrava il difetto alla
giunzione miotendinea, l’iperemia del muscolo e l’estremità
tendinea. Il ventre muscolare del capo lungo del bicipite
appariva maggiormente ecogeno rispetto a quello del capo
breve producendo un aspetto “bianco e nero” (Fig. 7-8).
Discussion
The rupture of the long head biceps (LHB) can be either
traumatic or spontaneously triggered by light weight lifting
in underlying degenerative conditions. [1] The LHB tendon
rupture can be diagnosed clinically as it produces a lump in
the lower part of the anterior surface of the upper arm,
known as the “Popeye sign”. There is also a limitation of
flexion and supination strength of the forearm. When the
tendon is partially ruptured, there is no retraction. The
diagnosis may be more challenging in some cases including
obese patients with thick arms. In cases like these and in
any patient with equivocal diagnosis, ultrasonography
should be used to reach an accurate, prompt and confident
diagnosis. [2,3]
Discussione: La rottura del capo lungo del bicipite (CLB) può
essere sia traumatica che indotta spontaneamente dal
sollevamento di pesi su un substrato degenerativo
preesistente. [1] La rottura del CLB può essere diagnosticata
clinicamente in quanto produce una bozzatura nella parte
distale della superficie anteriore del braccio conosciuta
come segno di “braccio di ferro”. E’ inoltre presente una
limitazione della forza in flessione e supinazione. Quando la
lesione è parziale non è presente retrazione. La diagnosi può
essere più complessa in alcuni casi come nei pazienti obesi o
con braccia particolarmente spesse. In questi casi, ed in
generale nei casi in cui la diagnosi non sia univoca, l’ecografia
dovrebbe essere utilizzata per raggiungere una diagnosi
accurata, sicura e rapida. [2,3]
ULTRASONOGRAPHIC IMAGING OF BICEPS TENDON RUPTURE
AT THE MYOTENDINOUS JUNCTION.
Ultrasonography demonstrates an “empty groove” when
the rupture occurs in an intra-articular level and the muscle
retracts distally. The “empty groove sign” is visible only in
acute cases, where fluid collection is also visible into the
sheath and the muscle belly maintains its normal
echotexture and has a fusiform shape. The stump of the
tendon can be seen as a hyperechoic structure with a
hypoechoic halo representing the fluid. The shrunk distal
tendon may be characterized by posterior acoustic
attenuation. Occasionally, debris in the sheath may make
the diagnosis of rupture difficult. In these cases,
identification of the myotendinous junction just below the
pectoralis major tendon suggests an intact LBH tendon.
[2,3]
In chronic cases, the torn LBH tendon can be replaced by
scar tissue whose ultrasonographic characteristics are
similar to tendon’s when seen on short-axis view. In such
cases, long-axis views demonstrate the lack of fibrillar
pattern. [4] Atrophy and fatty infiltration may render the
torn and retracted belly echogenic compared to the normal
one, giving the “black and white appearance” on transverse
views. [2,3]
In rare cases, the biceps tendon may be torn at the level of
the myotendinous junction, as it was the case in the patient
presented. The tendon remains then inside the groove,
giving a normal appearance. [2] In other, even rarer
traumatic cases, the rupture may affect the LHB belly itself.
This kind of rupture is often seen in soldiers performing
parachute jumps but can also affect civilians. The peripheral
tendon connecting the merged bellies of the biceps to the
radial tuberosity can also be ruptured, in only 3% of all
biceps tendon tears. [5,6] In conclusion, ultrasonography is
simple, reproducible and easily performed for the diagnosis
of LHB rupture. It has a reported sensitivity of 88%,
specificity of 98%, positive predictive value of 88%, negative
predictive value of 98% and accuracy of 97%. [7]
L’IMAGING ECOGRAFICO DELLA ROTTURA DEL TENDINE DEL
BICIPITE ALLA GIUNZIONE MIOTENDINEA
L’ecografia dimostra la “doccia vuota” quando la rottura si
realizza in sede intrarticolare e il muscolo si retrae
distalmente. Il segno della “doccia vuota” è visibile
unicamente nei casi acuti, quando la raccolta fluida è visibile
entro la guina e il ventre muscolare mantiene la sua normale
ecostruttura e la forma rimane fusata. Il moncone tendineo
può essere visto come una struttura iperecogena con un
alone ipoecogeno rappresentato dal fluido. Il moncone
distale può essere caratterizzato da un’attenuazione
posteriore del fascio ultrasonoro. In alcuni casi la presenza di
detriti entro la guaina può rendere difficile la diagnosi di
rottura. In questi casi l’identificazione della giunzione
miotendinea appena al di sotto del tendine del muscolo
grande pettorale suggerisce la presenza di un CLB non
lesionato. [2-3]
Nei casi di lesione cronica il tendine del CLB può essere
sostituito da tessuto cicatriziale le cui caratteristiche
ecografiche sono simili a quelle del tendine quando
visualizzato sull’asse breve. In questi casi la visualizzazione
sull’asse lungo dimostra l’assenza dell’aspetto fibrillare. [4]
L’atrofia e l’infiltrazione adiposa posso rendere il ventre
muscolare lesionato e retratto ecogeno rispetto a quello
normale dando quindi il tipico aspetto “bianco e nero” nelle
scansioni trasverse. [2,3]
In rari casi il tendine del bicipite può lesionarsi a livello delle
giunzione miotendinea, come è avvenuto nel caso qui
riportato. Il tendine rimane quindi entro la doccia bicipitale,
simulando l’aspetto normale. [2] In altri, ancor più rari, casi
di rottura traumatica la lesione può interessare il ventre
muscolare stesso del CLB. Questo tipo di rottura è spesso
vista nei soldati paracadutisti che realizzano dei lanci ma può
essere riscontrata anche tra i civili. Anche il tendine distale
che connette i ventri muscolari riunitisi alla tuberosità
radiale può rompersi ma questa evenienza rappresenta solo
il 3% di tutte le lesioni. [5,6] In conclusione l’ecografia è una
tecnica semplice e riproducibile per la diagnosi di rottura del
CLB. In letteratura viene riportata una sensibilità dell’88%,
una specificità del 98%, un valore predittivo positivo
dell’88% e un valore predittivo negativo del 98% con
un’accuratezza del 97%. [7]
ULTRASONOGRAPHIC IMAGING OF BICEPS TENDON RUPTURE
AT THE MYOTENDINOUS JUNCTION.
L’IMAGING ECOGRAFICO DELLA ROTTURA DEL TENDINE DEL
BICIPITE ALLA GIUNZIONE MIOTENDINEA
References
1. Russo A. Spontaneous rupture of biceps brachii tendon;
ultrasound diagnosis in emergency, apropose of two cases.
Updating results of surgical repair. Ann Ital Chir 2008; 79(4):303-9.
References
1. Russo A. Spontaneous rupture of biceps brachii tendon;
ultrasound diagnosis in emergency, apropose of two cases.
Updating results of surgical repair. Ann Ital Chir 2008; 79(4):303-9.
2. Bianchi S, Martinoli C. Shoulder. In: Ultrasound of the
Musculoskeletal System. Edited by Baert AL, Knauth M, Sartor K.
Berlin: Springer, 2007, pp189-331.
2. Bianchi S, Martinoli C. Shoulder. In: Ultrasound of the
Musculoskeletal System. Edited by Baert AL, Knauth M, Sartor K.
Berlin: Springer, 2007, pp189-331.
3. Fornage BD, Rifkin MD. Ultrasound examination of tendons.
Radiol Clin North Am 1988; 26(1):88-107.
4. Daenen B, Houben G, Bauduin E, Lu KV, Meulemans JL.
Ultrasound of the shoulder. JBR-BTR 2007; 90(5):325-337.
3. Fornage BD, Rifkin MD. Ultrasound examination of tendons.
Radiol Clin North Am 1988; 26(1):88-107.
4. Daenen B, Houben G, Bauduin E, Lu KV, Meulemans JL.
Ultrasound of the shoulder. JBR-BTR 2007; 90(5):325-337.
5. Wilson DJ, Parada SA, Slevin JM, Arrington ED. Intrasubstance
ruptures of the biceps brachii: diagnosis and management.
Orthopedics 2011; 34(11):890-6.
5. Wilson DJ, Parada SA, Slevin JM, Arrington ED. Intrasubstance
ruptures of the biceps brachii: diagnosis and management.
Orthopedics 2011; 34(11):890-6.
6. Miller TT, Adler RS. Sonography of Tears of the Distal Biceps
Tendon. AJR Am J Roentgenol 2000; 175(4):1081-6.
6. Miller TT, Adler RS. Sonography of Tears of the Distal Biceps
Tendon. AJR Am J Roentgenol 2000; 175(4):1081-6.
7. Skendzel JG, Jacobson JA, Carpenter JE, Miller BS. Long Head of
Biceps Brachii Tendon Evaluation: Accuracy of Preoperative
Ultrasound. AJR Am J Roentgenol 2011; 197(4):942–948.
7. Skendzel JG, Jacobson JA, Carpenter JE, Miller BS. Long Head of
Biceps Brachii Tendon Evaluation: Accuracy of Preoperative
Ultrasound. AJR Am J Roentgenol 2011; 197(4):942–948.
Figure legends
Fig. 1: Photograph showing the “popeye’s” sign (arrowhead).
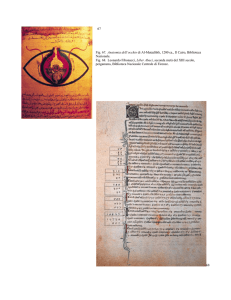
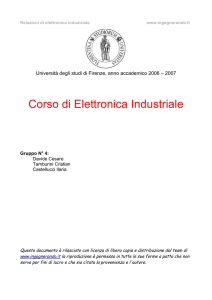
Fig. 2: Longitudinal power Doppler imaging scan over the tendon
showing the point of rupture (asterisk). The sheath appears
distended and fluid filled distally to the rupture. There are only
limited blood flow signals in the muscle and tendon ends. (H:
humerus).
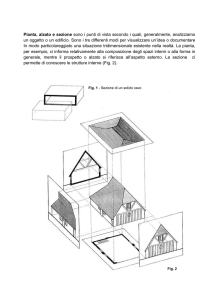
Fig. 3: Short-axis view of the myotendinous junction of the LHB in
relation to the pectoralis major tendon insertion (arrowhead). The
biceps sulcus appears filled with the torn biceps tendon or debris.
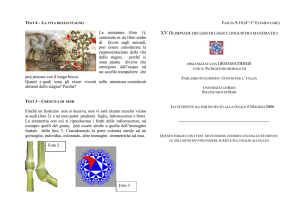
Fig. 4: Longitudinal extended field-of-view image of the LHB
tendon inside its groove and cephalad to the rupture site
(arrowheads). Arrow showing the site of rupture. (D: deltoid
muscle, H: humerus).
Fig. 5: Long-axis extended field-of-view image over the LHB belly
and distally to the rupture site (arrow) during relaxation. The belly
appears with normal echogenicity.
Fig. 6: Dynamic longitudinal extended field-of-view image of the
LHB belly during contraction. Note the increased length of defect
(arrows). The belly exhibits a global appearance when contracted.
Fig. 7: Long axis view of the proximal LHB tendon on follow-up
showing increased vascularity with power Doppler Imaging.
Fig. 8: Transverse extended field-of-view at the level of distal arm
showing the “black and white” appearance of the muscles. Thin
arrow showing the short head of the biceps belly, thick arrow
showing the LHB belly. (H: humerus).
Legenda delle figure
Fig. 1: La fotografia mostra il segno di “braccio di ferro” (testa di
freccia).
Fig. 2: Scansione longitudinale Power-Doppler a livello del tendine
che mostra la sede della rottura (asterisco). La guaina è distesa da
fluido che distalmente riempie la sede della rottura. Sono presenti
solo minimi segnali di flusso a livello del ventre muscolare e del
moncone tendineo (H: omero).
Fig. 3: Scansione assiale della giunzione miotendinea del CLB nel
punto in cui entra in relazione con l’inserzione del tendine del
muscolo grande pettorale (testa di freccia). Nel solco bicipitale è
presente il moncone tendineo o detriti.
Fig. 4: Scansione longitudinale con campo di vista esteso del
tendine del capo lungo del bicipite (testa di freccia) all’interno del
solco in sede craniale rispetto alla sede di lesione. La freccia
mostra la sede di lesione. (D: muscolo deltoide, H: omero).
Fig. 5: Scansione in asse lungo con campo di vista esteso del
ventre muscolare del CLB e distalmente del sito di rottura, in fase
di rilassamento. Il muscolo presenta ecogenicità normale.
Fig. 6 Scansione longitudinale con campo di vista esteso del ventre
muscolare del CLB durante la contrazione. Notare l’aumento di
ampiezza del difetto (frecce). Il ventre muscolare appare
maggiormente arrotondato quando contratto.
Fig. 7: Scansione in asse lungo della porzione prossimale del
tendine del CLB al follow-up che dimostra un incremento della
vascolarizzazione al Power-Doppler.
Fig. 8: Scansione trasversa con campo di vista esteso a livello della
porzione distale del braccio che dimostra l’aspetto “bianco e nero”
dei ventri muscolari. La freccia sottile indica il ventre muscolare
del capo breve mentre la freccia spessa indica il ventre del CLB. (H:
omero).
ULTRASONOGRAPHIC IMAGING OF BICEPS TENDON RUPTURE
AT THE MYOTENDINOUS JUNCTION.
L’IMAGING ECOGRAFICO DELLA ROTTURA DEL TENDINE DEL
BICIPITE ALLA GIUNZIONE MIOTENDINEA