La Consulenza Genetica ed i test genetici
nella pratica clinica
Siena, Giovedì 24 Settembre 2009
La Sindrome di Epstein, la Sindrome di
Fechtner e le sindromi correlate
Marco Seri
Un po’ di storia……
FECHTNER SYNDROME
Cataracts
Nephritis
Deafness
Macrothrombocytopenia
Leukocyte inclusion bodies
FECHTNER SYNDROME
Cataracts
Nephritis
Deafness
Macrothrombocytopenia
Leukocyte inclusion bodies
MAY-HEGGLIN ANOMALY
SEBASTIAN SYNDROME
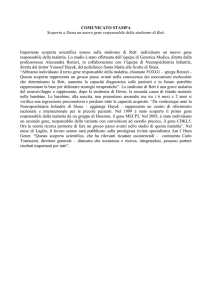
In MHA, the “Döhle-like bodies” consist of an amorphous area of cytoplasm
containing clusters of ribosomes oriented along parallel microfilaments
In SBS, the “Döhle-like bodies” are composed of highly dispersed
filaments and few ribosomes
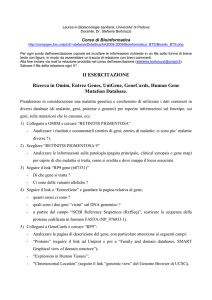
D22S278
D22S283
D22S426
Lod score
θ=0.0
4.10
q11-q13
APOL2
MYH9
TXN2
E1F3S7
CACNG2
D22S283
D22S1173
D22S683
D22S278
TNF-inducible
protein CG12-1
D22S426
APOL
dJ 1 1 1 9 A 7 .3
dJ 1 1 1 9 A 7 .5
FTNS/MHA critical region: ca. 480000 bp
Cen
Tel
Z82217
Z95114
AL031426
Z82215
AL022302
AL022313
AL031845
Z70289
Il gene MYH9 codifica per la catena pesante della miosina non
muscolare di tipo IIA (NMMHC-IIA) che è espressa in alcuni
tessuti quali piastrine, rene, leucociti e coclea.
Altre miosine non convenzionali sono associate a malattie
nell’uomo che mostrano sordità o difetti dell’occhio.
Miosina VIIA
Usher syndrome type IB
(sordità congenita, areflessia vestibolare e
retinite pigmentosa progressiva)
DFNB2 (sordità recessiva non sindromica)
Miosina XV
DFNB3 (sordità recessiva non sindromica)
Miosina VI
Snell's waltzer deafness: modello murino
DFNA22 (sordità dominante non sindromica)
Nephritis
Deafness
Macrothrombocytopenia
Leukocyte inclusion bodies
MAY-HEGGLIN ANOMALY
SEBASTIAN SYNDROME
EPSTEIN
SYNDROME
FECHTNER SYNDROME
Cataracts
Sarcomeric, smooth muscle and nonmuscle class II myosins
Exameric enzymes
light chain
heavy chain
COOH
COOH
Motor domain
• ATP hydrolysis
• actin binding
Coiled coil
• assembly of bipolar myosin filaments
MYH9-RELATED DISEASE
Cataracts
Nephritis
Deafness
Macrothrombocytopenia
Leukocyte inclusion bodies
MAY-HEGGLIN ANOMALY
SEBASTIAN SYNDROME
EPSTEIN
SYNDROME
FECHTNER SYNDROME
DFNA17
•Recurrent mutations (codons 96, 702, 1155, 1165, 1424, 1841,
1933) represents 88% of all mutations identified up to date in the
MYH9 gene.
•Deletions and missense or frameshift mutations resulting in a
truncated protein have never been described.
•The presence of missense or frameshift mutations have been
described only in the last exon, coding for the C-terminal tail which
is essential to assemble the molecule in bipolar filaments,
suggesting that the dominant negative effect is the pathogenetic
mechanism.
•However, it is still being debated if the pathogenetic mechanism is
a Dominant Negative effect due to the altered dimer formation or
rather if it is Haploinsufficiency.
A locus presents Haploinsufficiency if more genic product than
the one obtained by a single gene allele is necessary for
the expression of the normal phenotype.
The Dominant Negative effect takes place when the genic product
of the mutated allele affects the function of the wild type one.
La patogenesi
Aploinsufficienza?
Effetto Dominante
Negativo?
Kunishima S et al. “Immunofluorescence analysis of neutrophil Nonmuscle
Myosin Heavy Chain-A in MYH9 disorders: association of subcellular
localization with MYH9 mutations” Laboratory Investigation (2003)
Deutsch S et al.”Asp1424Asn MYH9 mutation results in an unstable protein
responsible for the phenotypes in May-Hegglin anomaly/Fechtner syndrome”
Hemostasis, Thrombosis, and Vascular Biology (2003)
Takubo T et al.”Expression of non muscle type myosin heavy polypeptide 9
(MYH9) in mammalin cells” European Journal of Histochemistry (2003)
Franke JD et al. “Rod mutations associated with MYH9-related disorders
disrupt non-muscle myosin-IIA assembly” Blood (2004)
Pecci A et al. “Pathogenetic mechanisms of hematological abnormalities of
patients with MYH9 mutations” Human Molecular Genetics (2005)
It seems that several genetic mechanisms take place in
the pathogenesis of the disease in different tissues.
The difficult accessibility of the other tissues involved in
the disease (e.g. inner ear and kidneys) makes it
extremely difficult to understand the molecular
mechanism leading to the disease.
giant platelets
leukocyte inclusions
thrombocytopenia
MYH9
deafness
cataracts
nephritis
Protocollo diagnostico
• Striscio di sangue
Immunoistochimica
mAb against
NMMHC-IIA
MGG
Co
ol
r
nt
ele
t
a
l
P
ts
ele
t
a
l
P
ts
Immunofluorescenza
A
B
Se positivo analisi degli esoni contenenti le
mutazioni ricorrenti, (1, 16, 24, 25, 26, 30,
38, 40) quindi analisi delle altre parti del
gene
Se negativo non viene effettuata la diagnosi
molecolare ma…..
…….è sempre importante inviare il paziente
alla CONSULENZA GENETICA
Acknowledge
University of Bologna
Dr E. Panza
Prof M.Seri
University of Pavia
Dr A. Pecci
Prof C. Balduini
University of Genova
Dr.ssa M. Marini
Prof R. Ravazzolo
University of Trieste
Dr.ssa F. Di Bari
Prof.ssa A. Savoia
Setting up an in vitro model to study the effect
of MYH9 mutations
CLONING OF THE ENTIRE MYH9 cDNA
SCHEMA CLONAGGIO MIOSINA 9
Frammento A
2338 bp
Frammento B
1675 bp
Aat II
Frammento C
1865 bp
Eco RI
MYH9 RT3
MYH9 RT2
MYH9 RT
NMMHC-IIA (red)
GST (green)
FTNS
EPTS
FTNS/EPTS
E1841K
R1933X
R702C
D1424Y
D1424N
R1165C
N93K A95T
T1155I
R705H
Del L1205
-Q1207
5828delG
E1945X
1
10
16
K371N
S96L
24
25
26
30
Del E1066 S1114P
-A1072
R1165L
38
40
5774delA 5779delC
R702H
D1424H
D1424H
Motor domain
light chains
MHA
SBS
MHA/SBS
DFNA17
Coiled coil
heavy chains
COOH
COOH
Transfection of COS cells with wild-type MYH9 cDNA
NMMHC-IIA (red)
Transfection of COS cells with D1424H MYH9 cDNA
NMMHC-IIA (red)
Transfection of COS cells with D1424H MYH9 cDNA
NMMHC-IIA (red)
Transfection of COS cells with D1424H MYH9 cDNA
NMMHC-IIA (red)
Cotransfection experiments with MYH9 WT and D1424H
FLAG (D1424H)
V5 (WT)
The co-trasfection, revealed by the double FLAG/V5 labelling is good
Flag-Tag
A
V5-Tag
B
x
C
D
Cotransfection experiments with MYH9 WT and D1424H
FLAG (D1424H)
V5 (WT)
FLAG (mutant) signal has a strong preferential localization in the sub-membrane region
rather than in the cytoplasm,
V5 (WT) signal has a more homogeneous distribution among the sub-membrane region
And the cytoplasm
TRANSFECTED CELLS
A
PERIPHERAL BLOOD
WILD-TYPE NMMHC-IIA
D
CO-TRANSFECTED CELLS
D1424H NMMHC-IIA
G
D1424H NMMHC-IIA
B
E
C
F
WILD-TYPE NMMHC-IIA
H
MERGING
I
In co-transfected cells the mutant MYH9 showed a
distribution similar to that observed in cells transfected
with mutant MYH9 alone, with part of the Flag signal
diffused in the cytoplasm and part organized in rod
like aggregates.
Aggregates were globally less frequent than in cells
transfected with D1424H cDNA alone.
Confocal analysis demonstrates that WT signal presented
a high degree of co-localization with the mutant signal
diffused in the cytoplasm, thus suggesting that transfected
WT and D1424H molecules interact in these cells.
These findings suggest that the NMMHC-IIA mutated in position
1424 is able to interact with the WT form in living cells, despite
part of the mutant protein precipitates in non functional aggregates.
The fact that NMMHC-IIA mutated in position 1424 retains the
ability to interact with WT protein represents the basis for it
to exert a dominant negative biochemical effect on the normal
protein.
E1841K
E1841K
FTNS
EPTS
FTNS/EPTS
R1933X
R702C
R1933X
R702C
D1424Y
D1424N
D1424N
R1165C
R1165C
N93K A95T
T1155I
R705H
Del L1205
-Q1207
5828delG
E1945X
1
10
16
K371N
S96L
24
25
26
30
Del E1066 S1114P
-A1072
R1165L
38
40
5774delA 5779delC
R702H
R702H
Motor domain
light chains
MHA
SBS
MHA/SBS
DFNA17
D1424H
D1424H
Coiled coil
heavy chains
COOH
COOH
Malattie Mendeliane
Malattie Multifattoriali
MYH9 is associated with nondiabetic end-stage renal disease
in African Americans (Nature Genetics 2008)
MYH9 is a major-effect risk gene for focal segmental
glomerulosclerosis (Nature Genetics 2008)
Genome-wide linkage analysis of serum creatinine in three
isolated European populations (Kidney International 2009)
Polymorphisms in the Nonmuscle Myosin Heavy Chain 9 gene
(MYH9) are associated with albuminuria in hypertensive
African Americans (American Journal of Nephrology 2009)
Polymorphisms in the Nonmuscle Myosin Heavy Chain 9 gene
(MYH9) are strongly associated to end stage renal disease
hystorically attribuited to hypertension in African Americans
(Kidney International 2009)
From Nat. Genet. 24:333-335; 2000
Figure 1
A
B
C
Two-Hybrid System
MYH9 (NMMHC-IIA) – MYH10 (NMMHC-IIB)
Future prospectives........
In collaboration with Professor Francesco Blasi, San Raffaele, Milano,Italy.
Deletion constructs
∆451X
W828X
Y1460X
R1933X
WT
light chains
Motor domain
Coiled coil
heavy chains
COOH
COOH
VECTORS, MUTANTS and MYH9 CLONES
WT
Entry Clone
201
(Kanamicina)
x
Entry Clone
207
(Gentamicina)
x
K371N
R702H
R702C
R1165C
x
x
-
x
D1424H
-
x
x
pDEST 27
GST
(Ampicillina)
x
x
x
E1945X
R1933X
-
x
x
x
x
pDEST-FLAG
(Kanamicina)
pDEST53
GFP
(Ampicillina)
E1841K
x
pDEST 26
6xHIS
(Ampicillina)
pcDNA3.1/nV5
DEST-V5
(Ampicillina)
D1424N
x
x
x
x
x
x
x
x
x
x
D1424H NMMHC-IIA
A
B
C
D
E
F
PERIPHERAL BLOOD
TRANSFECTED CELL LINES
WILD-TYPE NMMHC-IIA
Panza E, Pecci A, Marini M, Giacopelli F, BozziV, Seri M,Balduini C, Ravazzolo R.
“Transfection of the mutant MYH9 cDNA reproduces the most typical cellular phenotype of MYH9-related
disease in different cell lines”
Pathogenetics 2008 Dec 1;1(1):5.
Cotransfection experiments with MYH9 WT and D1424H
FLAG (mutant)
V5 (WT)
In some cells the FLAG (mutant) signal has a high irregular distribution, and form
structures similar to filaments and spots, while the V5 (WT) signal is more
regularly distributed (microscopic spots uniformly distributed in the cytoplasm).
Cotransfection experiments with MYH9 WT and D1424H
FLAG (mutata)
V5 (WT)
Some aggregates are evident with anti-FLAG (mutant) antibody;
these aggregates are more evident in FLAGpos / V5neg cells or
in cells with weak V5 signal, where WT has not been trasfected or seems to be poorly
expressed.
Cotrasfection experiments with MYH9 WT and D1424H
FLAG (mutant)
V5 (WT)
Some feeble aggregates are evident with the antibody anti-FLAG (mutant) also in some
cells co-transfected FLAGpos / V5pos with strong V5 signal;
In these cells aggregates are not visible with anti-V5 (WT) antibody.
Cotransfection experiments with MYH9 WT and D1424H
FLAG (mutant)
V5 (WT)
Cotransfection experiments with MYH9 WT and D1424H
FLAG (mutant)
V5 (WT)
Cotransfection experiments with MYH9 WT and D1424H
FLAG (mutant)
V5 (WT)
Cotransfection experiments in COS7 cell lines
MYH9 WT
MYH9 D1424H
GST signal is not a good tag to follow WT MYH9
6xHis is not a good tag to follow mutant MYH9
Cotransfection experiments in COS7 cell lines
MYH9 WT
MYH9 D1424H
V5 is good to follow WT MYH9
but still, the overall system is not good enough......
Looking for a new expression vector........
Gateway Converting System Kit
FLAG
pCMV-FLAG-DEST
The genotype-phenotype correlation leads to the concept that
the MYH9-RD phenotype results from the joint effect of MYH9
mutations and unknown enviromental and/or genetic factors, such as
multiple gene products.
21 Families
6FTNS
6EPTS
4MHA
1SBS
4MHA/SBS
47 Patients
38 familial cases
9 sporadic
16FTNS
6EPTS
9MHA
3SBS
4MHA/SBS
3FTNS
3EPTS
19FTNS
1MHA
2MHA/SBS
8EPTS
10MHA
3SBS
6MHA/SBS
MYH9 mutations are present in 19 out of 21 patients analyzed
MYH9 Mutations
Exon
N93K
1
R702C
16
R702H
16
K910Q
21
Del E1066-A1072
24
T1155I
25
R1165C
26
D1424H
30
D1424H
30
E1841K
38
1 case
R1933X
40
1 case
E1945X
40
1 case
* same patient
FTNS
EPTS
MHA
SBS
MHA/SBS
1 case
1 case
2 case
1 case
1 case
3 cases
1 caso*
1 case
1 case
1 case
3 cases*
1 case
FTNS
EPTS
FTNS/EPTS
E1841K
R1933X
R702C
D1424Y
D1424N
R1165C
N93K A95T
T1155I
R705H
Del L1205
-Q1207
5828delG
E1945X
1
10
16
K371N
S96L
24
25
26
30
Del E1066 S1114P
-A1072
R1165L
38
40
5774delA 5779delC
R702H
D1424H
Motor domain
light chains
MHA
SBS
MHA/SBS
DFNA17
Coiled coil
heavy chains
COOH
COOH
•Alcune mutazioni sono ricorrenti
96 (S->L); 702 (R->C, R->H); 1155 (T->I);
1165 (R->C, R->L); 1424 (D->H, D->N); 1841 (E->K);
1933 (R->X)
•Mutazioni Nonsenso e frameshift colpiscono solo l’ultimo
esone del gene MYH9 gene (R1933X, E1945X, 5774delA,
5779delC and 5828delG)
•Solo delezioni “in frame” di pochi aminoacidi sono state
identificate nel gene MYH9 (del L1205-Q1207; del
E1066-A1072 )
R1933X
E1841K
R702C
R702H
D1424H
T1155I
MHA-SBS
FTNS-EPTS
MHA-SBS
R1165C
geni
modificatori
FTNS-EPTS
mAb against
NMMHC-IIA
MGG
Co
ol
r
nt
op h
r
t
u
Ne
ils
ets
l
e
t
Pla
Neu
ils
h
p
tro
ets
l
e
t
Pla
A
B
C
E
F
G
•Pertanto la classificazione di FTNS, EPTS, MHA and SBS come
malattie separate appare non corretta ed i criteri clinici utilizzati
per questa classificazione vanno riconsiderati.
•Queste malattie mostrano uno spettro continuo di sintomi dalla
macrotrombocitopenia, alle inclusioni nei polimorfonucleati fino alla
sordità neurosensoriale, alla cataratta ed infine alla nefrite.
•Noi proponiamo così che queste patologie siano considerate come
un’unica entità clinica da chiamare “MYH9-related disease”.
•L’espressività variabile della malattia può essere poi spiegata
dall’effetto congiunto di specifiche mutazioni, di fattori ambientali
così come dalla presenza di "modifier genes”.
MYH9-RELATED DISEASE
Cataracts
Nephritis
Deafness
Macrothrombocytopenia
Leukocyte inclusion bodies
MAY-HEGGLIN ANOMALY
SEBASTIAN SYNDROME
EPSTEIN
SYNDROME
FECHTNER SYNDROME
DFNA17
•Per meglio definire lo spettro delle malattie da mutazioni nel gene
MYH9, abbiamo studiato 3 famiglie aggiuntive che mostrano
fenotipi caratterizzati da trombocitopenia associata a vari livelli
con sordità, anomalie oculari e nefrite e pertanto in parte
sovrapponibili al quadro clinico presente nei pazienti con mutazioni
nel gene MYH9.
•L’analisi di linkage e/o l’analisi di sequenza ha escluso un
coinvolgimento del gene MYH9 come responsabile delle malattie
presenti in queste famiglie.
Macrothrombocytopenia
Hearing loss
Macrothrombocytopenia
Bilateral Cataracts
Hearing loss
Macrothrombocytopenia
Hearing loss
Nephritis
•Infine abbiamo raccolto un gruppo di 10 pazienti Alport nei quali
era stata ipotizzata una trasmissione autosomica dominante e
senza mutazioni nei geni del collagene di tipo 4 (COL4).
•L’analisi di questi casi tramite sequenziamento diretto della
regione codificante del gene MYH9 ci ha consentito di escludere un
coinvolgimento di questo gene nella patogenesi delle forme
dominanti di Sindrome di Alport.
•Tutti questi dati dimostrano che le malattie da mutazioni nel gene
MYH9 presentano un fenotipo definito che ha come caratteristica
fondamentale la presenza delle inclusioni nei leucociti rilevabili
attraverso la microscopia ottica o tramite esperimenti di
immunocitochimica.
Cosa stiamo facendo:
Sistema del doppio ibrido per trovare proteine ineragenti con la MYH9
Sistema del doppio ibrido mirato per proteine candidate
Esperimenti di coimmunoprecipitazione
Esperimenti di trasfezione del gene MYH9 wild-type e mutato
Studi di immunocitochimica su tessuti di pazienti
Modello animale
CLONAGGIO cDNA MIOSINA NON MUSCOLARE 9
NMMHC-A (red)
GST (green)
Transfection of COS cells with wild-type MYH9 cDNA
NMMHC-A (red)
Transfection of COS cells with wild-type MYH9 cDNA
NMMHC-A (red)
Transfection of COS cells with D1424H MYH9 cDNA
NMMHC-A (red)
Transfection of COS cells with D1424H MYH9 cDNA
NMMHC-A (red)
Transfection of COS cells with D1424H MYH9 cDNA
NMMHC-A (red)
A
C
B
D
E
G
F
H
A
B
C
D
•Il gene codificante per la podocina (NPHS2) è stato
recentemente identificato come responsabile di una
sindrome nefrosica autosomica recessiva resistente agli
steroidi.
•Il gene NPHS1 che codifica per la nefrina è stato
identificato essere coinvolto nella forma congenita di
sindrome nefrosica del tipo Finnico.
•La nefrina è il componente maggiore dello "slitdiaphragm" presente tra i processi interdigitati dei
podociti ed è stato ipotizzato che questa proteina è
importante per mantenere la struttura di questi processi.
•Recentemente è stato dimostrato che la nefrina
rappresenta una molecola di segnale ed i segnali indotti
dalla nefrina sono enormemente amplificati dalla podocina
che si lega alla coda citoplasmatica della nefrina.
•Infine è stato dimostrato di recente che la nefrina ancora
lo "slit-diaphragm" all'actina nel citoscheletro
•Queste due proteine giocano così un ruolo cruciale nella
funzione di filtrazione della barriera glomerulare e quando
mutate determinano una disfunzione del podocita e la
presenza di proteinuria.
NPHS2P
1- Intron 1 (301-309)
2- 951T>C
4- 1038A>G
71
TC
AA
79
TC
AA
37
TT
AA
77
TT
AA
7 7
C T
A A
73
CC
AA
37
CT
AA
77
TT
AA
77
CT
AA
37
CT
AA
37
CT
AA
77
TT
AA
77
TT
AA
77
TT
AA
77
TT
AA
77
TT
AA
77
TT
AA
73
CC
AG
79
CC
AA
77
TT
AA
37
CT
GA
Marco Seri
Roberto Cusano
Emanuele Panza
Monica Marini
Roberto Ravazzolo
Simone Gangarossa
Bianca Rocca
Raffaele Landolfi
Nicola Bizzarro
Filomena Di Bari
Anna Savoia
Alessandro Pecci
Patrizia Noris
Umberto Magrini
Carlo L. Balduini
Maria Savino
Maria Del Vecchio
Maria d’Apolito
Leopoldo Zelante
Gianluca Caridi
Gian Marco Ghiggeri
Paola Malatesta
Maria Capria
Pasi A. Koivisto
Ilaria Meloni
Alessandra Renieri
Luisa Murer
Giovanni Banfi
Michele Purrello
Carmine Pecoraro
Saverio Sartore
Achille Iolascon
A
B
Normal PMN
PMN with
Dohle-like
body
Normal platelets
C
Giant
platelet
D
Myh9
Myh10
Esempio 1. L’anticorpo anti-Myh9e quello anti-Myh10 sembrano riconoscere due sistemi di filamenti apparentemente differenti. Myh9 forma
filamenti grossolani uniformemente distribuiti in tutto il citoplasma della cellula, dalla regione perinucleare a quella corticale, dove
definiscono bene i confini cellulari; appaiono orientati lungo l’asse longitudinale dei prolungamenti e lungo le linee di forza. Myh10 forma
filamenti più sottili, che appaiono differenti innanzitutto perché possono essere orientati in maniera diversa, come nel nella parte inferiore della
cellula; inoltre sono presenti solo in alcune zone di citoplasma e non disegnano mai l’intero profilo della cellula – in particolare non sono mai
presenti fino alla zona corticale, che è sempre delimitata da Myh9.
La sovrapposizione dei due segnali sullo stesso piano dimostra meglio questi aspetti; si osserva come il segnale rosso e quello verde
siano in parte separati, me si intuiscono anche dei punti di sovrapposizione, contrassegnati da un segnale giallo.
Esempio 2. Idem. Notare come Myh9 disegni sempre bene il profilo e l’impalcatura della cellula e Myh10 corra solo in alcune
zone di citoplasma
Esempio 2, sovrapposizione, idem.
y
x
Esempio di proiezione ortogonale della fluorescenza rilevata su un determinato piano confocale sull’asse z. A destra della linea
tratteggiata è riportata la proiezione della fluorescenza rilevata lungo la linea centrale verticale sull’asse y (in pratica x e z sono fisse,
viene rilevata la fluorescenza lungo y); sotto la linea tratteggiata è riportata la proiezione della fluorescenza rilevata lungo la linea cen
-trale orizzontale sull’asse x (z e y fisse).
Si osservi come sono presenti zone di segnale rosso (filamenti Myh9), zone di segnale verde (filamenti Myh10) zone buie (spazio fra
i filamenti), ma anche zone con un chiaro segnale giallo (zone di colocalizzazione), indicate dalle frecce.
Altro esempio, idem.
Altra metodica per effettuare lo studio di colocalizzazione.
Tracciando una retta su un piano confocale viene
rilevata e confrontata l’intensità di segnale lungo la
retta per ciascun canale.
Qui si vede benissimo che su questo piano i due
maggiori picchi di fluorescenza nel verde - che
identificano due singole fibre di myh10 che passano
sul piano-, corrispondono con precisione nanometrica
ad altrettanti picchi di fluorescenza nel rosso,
identificando quindi due punti in cui le due strutture
vengono a contatto.
An accurate clinical re-evaluation of patients allows to observe that
patients carrying MYH9 mutations show a continuous spectrum of
clinical manifestation without evidence to support the differentiation in
distinct diseases.
The only two findings observed in all patients are the
macrothrombocytopenia and the abnormal distribution of NMMHC-IIA
within leukocytes.
mAb against
NMMHC-IIA
MGG
Co
ol
r
nt
ets
l
e
t
Pla
ets
l
e
t
Pla
Biochemical mechanisms through which mutations affect
the NMMHC-IIA function are not completely understood.
About 70% of the families have mutations in the C-terminal tail
and 88% of them affect only 4 residues (1165, 1424, 1841, 1933)
representing less than 1% of all the possible residues involved.
No consistent correlations have been identified between the 27
different MYH9 mutations identified so far and the variable
clinical evaluation of the disease.
Understanding genotype-phenotype correlation
Collection of new cases
“Italian registry for MYH9-Related Disease”
Pavia, Italy.
Molecular analysis of MYH9 exon 1, 15, 16, 25, 26, 30, 38, 40.
Bologna, Italy.
150 cases up to date (February 2008)
This study included 108 patients with MYH9-RD confirmed by molecular
analysis, diagnosed by the collaborative groups
from Junuary 2001 to December 2006.
Five new mutations identified; three missense and two single base deletions
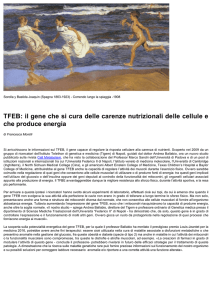
•La Sindrome di Fechtner (FTNS; MIM 153640) è una malattia
autosomica dominante descritta per la prima volta da Peterson
et al. (1985) che è stata considerata come una variante della
Sindrome di Alport.
•Infatti è caratterizzata da nefrite, sordità neurosensoriale ed
anomalie dell’occhio ma mostra anche caratteristiche aggiuntive
come la macrotrombocitopenia e corpi inclusi all’interno dei
polomorfonucleati chiamati “Döhle-like bodies”.
•L’anomalia di May-Hegglin (MHA; OMIM 155100) condivide
con la FTNS la triade clinica di trombocitopenia, piastrine
giganti e le caratteristiche inclusioni leucocitiche.
•La Sindrome di Sebastian (SBS; MIM 605249) è
caratterizzata dalle stesse alterazioni ematologiche ma si
differenzia dalla MHA sulla base delle immagini
ultrastrutturali dei “Döhle-like bodies”.
MHA/SBS
FTNS
E1841K
N93K
R702C
R1165C
D1424H
1
16
26
30
Motor domain
Coil coiled domain
38
R1933X
40
ACD
Assembly competence domain
K
Missense
C
C
H
K
HsnmIIa
XlnmIIa
RnnmIIa
RnNeur
GgnmII
(P35579)
(AAC83556)
(AAA74950)
(S21801)
(P14105)
93
702
1165
1424
1841
|
|
|
|
|
--ELTCLNEASVL---VLEGIRICRQG---ELRSKREQEVN---QQELDDLLVDL---QVRRTEKKLKD---ELACLNEASVL---VLEGIRICRQG---ELRTKREQEVT---QQELDDISVDL---QVRRTEKKLKD---ELTCLNEASVL---VLEGIRICRQG---ELRSKREQEVS---QQELDDLLVDL---QVRRAEKKLKD---ELTCLNEASVL---VLEGIRICRQG---ELRSKREQEVN---QQELDDLLVDL---QVRRTEKKLKD---ELTCLNEASVL---VLEGIRICRQG---ELRSKREQEVT---QQELDDIAVDL---QVRRAEKKLKD--
HsnmIIb
XlnmIIb
RnnmIIb
BtnmIIb
(P35580)
(AAA49915)
(AAF61445)
(BAA36494)
--ELTCLNEASVL---VLEGIRICRQG---ELRTKREQEVA---QQELDDLTVDL---LVRRTEKKLKE---ELTCLNEASVL---VLEGIRICRQG---ELRTKREQEVA---QQELDDLMVDL---LVRRTEKKLKE---ELTCLNEASVL---VLEGIRICRQG---ELRTKREQEVA---QQELDDLTVDL---LVRRTEKKLKE---ELTCLNEASVL---VLEGIRICRQG---ELRTKREQEVA---QQELDDLLVDL---LVRRTEKKLKE--
GgsmII
OcsmII
(P10587)
(P35748)
--ELTCLNEASVL---VLEGIRICRQG---ELRAKREQEVT---QQELDDLVVDL---TLRQKDKKLKD---ELTCLNEASVL---VLEGIRICRQG---ELRAKREQEVT---QQELDDLVVDL---ALKQRDKKLKE--
DmnmII
(Q99323)
--ELTCLNEASVL---VLEGIRICRQG---ELRSKREQELA---QSELEDATIEL---ANRKMDKKIKE--
Cenmy1
Cenmy2
(CAA99841)
(AAA83339)
--MLTCLNEASVL---VLEGIRICRQG---QLKAKRDEEYA---IQEAEDVQKEL---TLRRMETKMAE---ELTYLNEASVL---VLEGIRICRQG---DLMSRKDEEVN---QQELEDSSMEL---AARRLEKRLND--
•La Sindrome di Epstein (EPTS-OMIM 153650) è una malattia
ereditaria che si differenzia dalla FTNS solo per l’assenza dei
“Döhle-like bodies” nei granulociti e per l’assenza della cataratta
bilaterale.
•Gli esperimenti di immunocitochimica hanno messo in evidenza dei
patterns di immunoreattività che è possibile correlare con le diverse
mutazioni nel gene MYH9.
•La mutazione D1424H è associata con un singolo aggregato di
medie/larghe dimensioni nel citoplasma dei granulociti talvolta
associato con alcuni aggregati minori. I pazienti che presentano
questa mutazione mostrano anche una distribuzione negativa ed
irregolare della miosina nelle piastrine.
•Al contrario, le mutazioni al codone 702, normalmente identificate
nei pazienti EPTS, determinano la presenza nei granulociti neutrofili
di diversi microaggregati di dimensioni molto piccole spiegando così
la difficoltà di rilevare la presenza delle inclusioni attraverso una
colorazione con May-Grünwald-Giemsa. Le piastrine dei pazienti che
presentano una mutazione al codone 702 mostrano un pattern
diffuso.
•Macrotrombocitopenia è sempre presente.
•Anche nei pazienti EPTS si dimostra tramite esperimenti di
immunocitochimica la presenza di aggregati di miosina nei
leucociti.
•La presenza di ipoacusia è stata accertata nei pazienti
indipendentemente dalla diagnosi iniziale di FTNS, EPTS or
MHA-SBS ed in particolare nel 82% dei pazienti affetti da SBS
o MHA.
•La cataratta bilaterale è stata identificata in 11 pazienti e
sorprendentemente in 3 pazienti con una diagnosi di MHA-SBS.
•Una proteinuria massiva associata a ESRF è stata rilevata in 5
pazienti FTNS ed in 2 EPTS. Tuttavia una microematuria
ricorrente e bassi livelli di proteinuria sono stati riscontrati
anche in casi MHA-SBS
•Le mutazioni ricorrenti (codoni 96, 702, 1155, 1165, 1424,
1841, 1933) rappresentano una percentuale dell’ 85% di tutte le
mutazioni fino ad oggi identificate nel gene MYH9.
•Delezioni e mutazioni nonsenso o frameshift che risultano in una
prematura terminazione della proteina MYH9 non sono mai state
descritte.
•La presenza di mutazioni nonsenso e frameshift solo nell’ultimo
esone codificante per la parte C-terminale della proteina che
contiene il dominio deputato ad assemblare le molecole di MYH9
in filamenti bipolari, suggeriscono come meccanismo patogenetico
un effetto dominante negativo.
•Tuttavia se il meccanismo patogenetico di queste malattie sia
determinato da un meccanismo dominante negativo causato dalla
alterata formazione di dimeri di miosina oppure dipenda da una
aploinsufficienza resta ancora da dimostrare.
Kunishima S et al. “Immunofluorescence analysis of neutrophil Nonmuscle
Myosin Heavy Chain-A in MYH9 disorders: association of subcellular
localization with MYH9 mutations” Laboratory Investigation (2003)
Deutsch S et al.”Asp1424Asn MYH9 mutation results in an unstable protein
responsible for the phenotypes in May-Hegglin anomaly/Fechtner syndrome”
Hemostasis, Thrombosis, and Vascular Biology (2003)
Takubo T et al.”Expression of non muscle type myosin heavy polypeptide 9
(MYH9) in mammalin cells” European Journal of Histochemistry (2003)
Franke JD et al. “Rod mutations associated with MYH9-related disorders
disrupt non-muscle myosin-IIA assembly” Blood (2004)
The work demonstrates that:
all subjects with mutations in the motor domain
of NMMHC-IIA present with severe thrombocytopenia and develop
nephritis and deafness before the age of 40;
while subjects with mutations in the tail domain have much lower risk of
noncongenital complications and significantly higher platelet counts.
Mutations at residue 1933 do not induce kidney damage or cataracts and
cause deafness only in the elderly;
mutations at residue 702 result in severe thrombocytopenia and produce
nephritis and deafness at a juvenile age;
alterations at residue 1424 or 1841 result in intermediate clinical pictures.
MYH9-related disease (MYH9-RD) is a rare autosomal
dominant disorder caused by mutation in MYH9, the gene
coding for the heavy chain of nonmuscle myosin IIA
(NMMHC-IIA).
light chains
Motor domain
Coiled coil
heavy chains
COOH
COOH
All patients present from birth with macrothrombocytopenia,
but in infancy or adult life some of them develop
sensorineural
deafness,
presenile
cataracts,
and/or
progressive nephritis leading to end-stage renal failure.