Epidemiologia, clinica e terapia della
Malattia da Virus Ebola
Prof. Francesco Castelli
Chair of Infectious Diseases
UNESCO Chair
University of Brescia (Italy)
Director,
WHO Collaborating Center
for TB/HIV co-infection
and TB elimination strategy
Presidente,
Società Italiana di
Medicina Tropicale e
Salute Globale
… it is time to close the book on
infectious diseases. The war
against pestilence is over…
William Stewart, Surgeon General
in a message to Congress, 1969
People are not just people.
They are an awful lot of microbes, too
90 percent of the cells in the body
are microbial and only the
remaining 10 percent are human
Fattori favorenti l’emergenza di nuove
infezioni
•
•
•
•
•
•
•
•
•
Crescita popolazione, urbanizzazione
Aumentata produzione animale
Alterazioni habitat vettori / animali
Mobilità umana, vettori, germi, reservoir animale
Modificazioni dell’ecosistema (deforestazione, clima, etc.)
Comportamento umano
Pressione farmacologica (uomo e animale)
Adattamento microbico
Bioterrorismo ?
Incremento demografico
Urbanizzazione
80% : Latina America, Northern America
73% : Europe
48% : Asia
64% by 2050
40% : Africa
56% by 2050
https://www.google.it/search?q=world+population+and+animal+production&newwindow=1&rlz=1C1GGGE_itIT459IT526&espv=2&tbm=isch&imgil=M_S
OiDQYxgpObM%253A%253B_w12vKrYX8d9rM%253Bhttp%25253A%25252F%25252Fna.unep.net%25252Fgeas%25252FgetUNEPPageWithArticleI
DScript.php%25253Farticle_id%2525253D92&source=iu&pf=m&fir=M_SOiDQYxgpObM%253A%252C_w12vKrYX8d9rM%252C_&usg=__hS0kEDZ29
zihAQOEWWGpxmdRPZ4%3D&biw=1093&bih=499&ved=0CE0Qyjc&ei=i_lUVP7bFZaxaf7fgrgN#facrc=_&imgdii=_&imgrc=M_SOiDQYxgpObM%253A
%3B_w12vKrYX8d9rM%3Bhttp%253A%252F%252Fna.unep.net%252Fgeas%252FarticleImages%252FOct-12-figure1.png%3Bhttp%253A%252F%252Fna.unep.net%252Fgeas%252FgetUNEPPageWithArticleIDScript.php%253Farticle_id%253D92%3B1509%3B973
Examples of recent emerging diseases
NATURE; Vol 430; July 2004; www.nature.com/nature
Geosentinel
http://healthmap.org/en/
Outbreak Detection and Response
without Preparedness
First
Case
Late
Detection
Delayed
Response
90
80
60
Opportunity
for control
50
40
30
20
10
0
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
Cases
70
Day
Outbreak Detection and Response
with Preparedness
Early
Detection
Rapid
Response
90
80
Potential
Cases Prevented
60
50
40
30
20
10
0
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
Cases
70
Day
Il mestiere del guardiabosco …
Malattia da Virus Ebola:
• le vecchie epidemie
• quadro epidemiologico attuale
• modalità trasmissione
• aspetti clinici
Flying along the Zaire River to Yambuku, DR
Congo (Zaire), October 1976
Epidemiologists in Yambuku, DR Congo
(Zaire), 1976
Peace Corps Volunteer, Joel Breman, Peter Piot, Pierre Sureau
Country
Dem. Rep. of Congo
Town
Yambuku
Cases
318
Deaths
280
Species
Zaire ebolavirus
Year
1976
South Sudan
Dem. Rep. of Congo
Nzara
Tandala
284
1
151
1
Sudan ebolavirus
Zaire ebolavirus
1976
1977
South Sudan
Gabon
Ivory Coast
Nzara
Mekouka
Tai Forest
34
52
1
22
31
0
Sudan ebolavirus
Zaire ebolavirus
Taï Forest ebolavirus
1979
1994
1994
Dem. Rep. of Congo
Kikwit
315
250
Zaire ebolavirus
1995
Gabon
Gabon
South Africa
Uganda
Gabon
Republic of Congo
Republic of Congo
Republic of Congo
South Sudan
Dem. Rep. of Congo
Mayibout
Booue
Johannesburg
Gulu
Libreville
Not specified
Mbomo
Mbomo
Yambio
Luebo
37
60
2
425
65
57
143
35
17
264
21
45
1
224
53
43
128
29
7
187
Zaire ebolavirus
Zaire ebolavirus
Zaire ebolavirus
Zaire ebolavirus
Zaire ebolavirus
Zaire ebolavirus
Zaire ebolavirus
Zaire ebolavirus
Zaire ebolavirus
Zaire ebolavirus
1996
1996
1996
2000
2001
2001
2002
2003
2004
2007
Uganda
Bundibugyo
149
37
Bundibugyo ebolavirus 2007
Dem. Rep. of Congo
Luebo
32
15
Zaire ebolavirus
2008
Uganda
Luwero District
1
1
Sudan ebolavirus
2011
Uganda
Kibaale District
11*
4*
Sudan ebolavirus
2012
Dem. Rep. of Congo
Isiro Health Zone
36*
13*
Bundibugyo ebolavirus 2012
Uganda
Luwero District
6*
3*
Sudan ebolavirus
2012
Malattia da Virus Ebola:
• le vecchie epidemie
• quadro epidemiologico attuale
• modalità trasmissione
• aspetti clinici
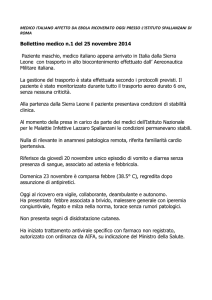
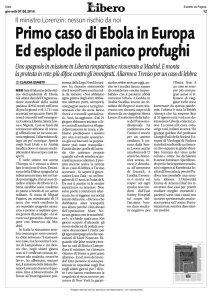
Attuale epidemia: paziente zero
Bimbo di 2 anni, originario del piccolo villaggio
di Guéckédou, nella Guinea sudorientale,
morto il 6 dicembre scorso e probabilmente
infettatosi mangiando la frutta non cotta
contaminata dai pipistrelli della frutta.
La particolare collocazione del villaggio, in una
regione lungo il confine tra Liberia, Sierra
Leone e la stessa Guinea, ha contribuito alla
creazione di corridoi iniziali di trasmissione
in questi tre Paesi.
I primi ad ammalarsi e morire sarebbero
stati i familiari del bimbo: la madre, la
sorellina di tre anni e la nonna. Due
partecipanti al funerale delle prime vittime
avrebbero poi contribuito alla trasmissione del
contagio ai loro rispettivi villaggi e da lì,
attraverso i parenti stretti e alcuni operatori
sanitari, ad altri centri.
Origine e diffusione dell’epidemia
monrovia
N Engl J Med 2014; 371:1481-1495. DOI:
10.1056/NEJMoa1411100
Le date «chiave» della epidemia
6 dicembre 2013 :
inizio della epidemia in Guinea Conakry
23 marzo 2014 :
l’OMS viene ufficialmente informata della
rapida evoluzione della epidemia di Ebola
8 agosto 2014 :
l’OMS dichiara la attuale epidemia di Ebola
una emergenza globale
17 settembre 2014 : le Nazioni Unite dichiarano Ebola in Africa
Occidentale una minaccia per la pace e la
sicurezza
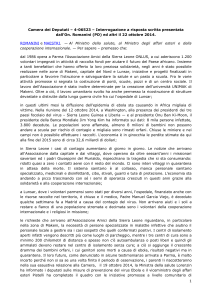
UK(29/12->)
Confirmed: 1 Deaths: 0
Contacts identified: ?
USA (1Texas- 1NY) (24/9->)
Total: 2+2 confirmed case
Deaths: 1
Contacts identified: 470
SENEGAL (20/8->19/10)
Total: 1 confirmed case
Deaths: 0
Contacts identified: 74
MALI (22/10->)
Confirmed: 7 Probable: 1
Deaths: 6
Contacts identified: 327
NIGERIA (20/7->20/10)
Total: 1 +19 clinical cases
Confirmed: 19 (Lagos 15, Port Harcourt 4)
Probable: 1
Deaths: 8 (7 confirmed, 1 probable)
ECDC 18 Dec 2014
Date of Evacuation Evacuated from Evacuated to
Profession
Status
02 August 2014
Liberia
Atlanta (USA)
Healthcare
worker
Discharged Yes
USA
05 August 2014
Liberia
Atlanta (USA)
Healthcare
worker
Discharged Yes
USA
06 August 2014
Liberia
Madrid (Spain)
Healthcare
worker
Death
Spain
24 August 2014
Sierra Leone
London (United Healthcare
Kingdom)
worker
27 August 2014
Sierra Leone
Hamburg
(Germany)
Epidemiologist Recovered Yes
Senegal
Omaha (USA)
Physician
Discharged Yes
(obstetrician)
USA
09 September 2014 Kenema, Sierra Atlanta (USA)
Leone
Physician
Discharged Yes
USA
14 September 2014 Sierra Leone
Leiden (the
Netherlands)
Healthcare
worker
Discharged No
Netherland
s
14 September 2014 Sierra Leone
Leiden (the
Netherlands)
Healthcare
worker
Discharged No
Netherland
s
19 September 2014 Liberia
Paris (France)
Healthcare
worker
Discharged Yes
France
22 September 2014 Sierra Leone
Madrid (Spain)
Healthcare
worker
Death
Yes
Spain
22 September 2014 Sierra Leone
Geneva
(Switzerland)
Healthcare
worker
Admitted
Unknow Non-Swiss
n
28 September 2014 Sierra Leone
Maryland (USA) Healthcare
worker
Admitted
Unknow USA
n
02 October 2014
Sierra Leone
Frankfurt
(Germany)
Healthcare
worker
Stable
Yes
02 October 2014
Liberia
Omaha (USA)
Cameraman
Discharged Yes
USA
06 October 2014
Sierra Leone
Oslo (Norway)
Healthcare
worker
Discharged Yes
Norway
08 October 2014
Liberia
Leipzig
(Germany)
Laboratory
worker
Death
Yes
Sudan
01 November 2014 Sierra Leone
Paris (France)
UN worker
Unknown
Yes
Sierra
Leone
15 November 2014 Sierra Leone
Nebraska (USA) Healthcare
worker
Death
Yes
USA
20 November 2014 Sierra Leone
Geneva
(Switzerland)
Healthcare
worker
Unknown
Yes
Cuba
21 November 2014 Mali
Madrid (Spain)
Healthcare
worker
Unknown
No
Spain
24 November 2014 Sierra Leone
Rome (Italy)
Healthcare
worker
Admitted
Yes
Italy
04 September 2014 Monrovia,
Liberia
Confirm Citizenship
Yes
Discharged Yes
UK
Uganda
Guinea
74 confirmed cases were reported in the 7 days to 4 January 2015
There is no discernible upward or downward trend.
However, EVD continues to spread geographically, with the western
prefecture of Fria reporting confirmed cases for the first time
19 districts have reported a confirmed or probable case in the 21
days to 4 January.
Liberia
Case incidence has declined from a peak of over 300 new confirmed cases
per week in August and September to 8 new confirmed cases and 40
probable cases in the 5 days to 2 January, 2015.
The district of Montserrado, which includes the capital Monrovia, continues
to account for most cases in the country, with 6 confirmed and 33 probable
cases reported in the 5 days to 2 January.
Sierra Leone
There are signs that case
incidence may have levelled off in
Sierra Leone, although with 248
new confirmed cases reported in
the week to 4 January 2015, it
remains by far the worst-affected
country at present.
Fattori che hanno favorito la
comparsa dell’epidemia
•
•
•
•
Commistione habitat uomo-animale
Crescita demografica ed inurbamento
Comportamenti tradizionali (lavaggio cadavere)
Assenza di immunità nella popolazione
Repubblica Democratica del Congo (ex-Zaire)
24 agosto 2014: notificata epidemia in RD Congo (Boende, prov. Equateur), causata da
variante diversa da quella dell’Africa occidentale ma sempre della specie Zaire
ebolavirus); al 7 ottobre: 69 pts con MVE (38 confermati, 28 probabili, 3 sospetti), 49
decessi, letalità del 74% tra casi probabili e confermati
N Engl J Med, October 15, 2014; DOI: 10.1056/NEJMoa1411099
Malattia da Virus Ebola:
• le vecchie epidemie
• quadro epidemiologico attuale
• modalità trasmissione
• aspetti clinici
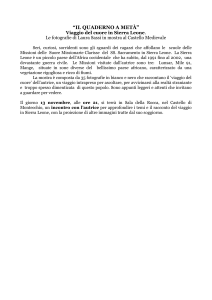
Towards detecting the natural host of the virus
Modalità contagio umano:
•Contatto con pipistrelli o
loro ambiente (grotte,
alberi da frutto infestati…)
•Contatto con animali
(primati o mammiferi)
(carcasse, sangue, carne
cruda) (luoghi infestati da
ratti)
•Contatto diretto o
indiretto con sangue o
liquidi biologici o tessuti di
malati o morti
No trasmissione per via aerea
No trasmissione da soggetti infetti asintomatici
Trasmissione interumana
TRASMISSIONE DA DROPLETS
• MANTENERE ALMENO 1
METRO DI DISTANZA
• MASCHERINA CHIRURGICA
• STANZA SINGOLA
• infezione meningococcica
• infezioni virali
• Inf. batteriche respiratorie
Carica infettante: 1-10 virus
(dati sperimentali su primati)
Rilevabilità di RNA di Virus Ebola dopo comparsa di sintomi
101 gg in seme
33
in secrezioni vaginali
29
nel retto
23
in urine
22
in tampone congiuntivale
21
in sangue
15
in latte
8
in saliva
6
su pelle
Numero di casi secondari prodotti da ogni caso (Ro)
1.81 (95% CI, 1.60 to 2.03) for Guinea
1.51 (95% CI, 1.41 to 1.60) for Liberia
1.38 (95% CI, 1.27 to 1.51) for Sierra Leone
Periodo incubazione: media 4-10, IC95% 2-21
Malattia da Virus Ebola:
• le vecchie epidemie
• quadro epidemiologico attuale
• modalità trasmissione
• aspetti clinici
Patogenesi
Poco nota:
Infezione di monociti, macrofagi e cellule dendritiche
Depressione immunità
Danno diretto del sistema vascolare
Danno diretto di cellule parenchimali di organi
bersaglio (fegato, milza, linfonodi, surrenali)
Danno da mediatori solubili (citochine, complemento)
risposta infiammatoria sistemica
Fase acuta:
-Replicazione virale e viremia
-Risposta immune
Ebola pathogenesis
Feldman et al., NATURE Reviews, 2003; 3: 677-85
Low risk of
transmission
High risk of
transmission
Filovirus activity among selected ethnic groups inhabiting the tropical
forest of equatorial Africa.
Johnson ED1, Gonzalez JP, Georges A.
Seroepidemiological surveys were conducted to determine the frequency and
distribution of filovirus activity among selected ethnic groups inhabiting the
tropical forests of the Central African Republic. 427 serum specimens were
collected from hunter-gatherers and subsistence farmers living in forest environs
in the Lobaye District south of the river Lobaye and west of the river Oubangui.
Striking serological evidence for filovirus activity was found in both
populations. Ebola virus appears to be the most active filovirus; 17.6% (75/427)
of the Lobaye survey population were seropositive forEbola virus reactive
antibody while 1.2% (5/427) were seroreactive with Marburg viral antigens.
Ethnic background appeared to be an important risk factor influencing filovirus
exposure in the forest communities. The filovirus antibody prevalence among 2140 years old male Aka Pygmy hunter-gatherers was significantly (P = 0.03) 3
times higher (37.5%) than that in similarly aged male Monzombo and Mbati
subsistence farmers (13.2%). Continued epidemiological investigations are
needed to define ethnic-related events influencing human filovirus activity in the
Congo basin of equatorial Africa.
Trans R Soc Trop Med Hyg. 1993 Sep-Oct;87(5):536-8
Treatment of Ebola
•
•
There are no approved treatments available for EVD.
Clinical management focus - supportive care of complications:
– hypovolemia, electrolyte abnormalities, hematologic abnormalities,
refractory shock, hypoxia, hemorrhage, septic shock, multi-organ failure,
and DIC.
•
Recommended care includes:
– volume repletion
– maintenance of blood pressure (with vasopressors if needed)
– maintenance of oxygenation
– pain control
– nutritional support
– treating secondary bacterial infections and pre-existing comorbidities
•
Among patients from West Africa, large volumes of intravenous fluids have often
been required to correct dehydration due to diarrhea and vomiting.
•
Several investigational therapeutics for Ebola virus disease are in development.
There are no approved vaccines available for EVD. Several investigational Ebola
vaccines are in development, and Phase I trials are underway for some vaccine
candidates.
Source: Centers for Disease Control and Prevention. http://www.cdc.gov/vhf/ebola/hcp/clinician-information-us-healthcaresettings.html Accessed Oct. 14, 2014
1) Mouse chimeric antibodies ch133, ch226
2) Ab cocktail: Zmab, MB-003
3) Zmapp: 1 Ab from MB-003 and 2 Abs from Zmab
Reversion of advanced Ebola virus disease in non
human primates with ZMapp.
Qiu X1, et al. Mapp
Biopharmaceutical Inc., San Diego, California 92121, USA.
……….
Here we show that a combination of monoclonal antibodies (ZMapp), optimized
from two previous antibody cocktails, is able to rescue 100% of rhesus macaques
when treatment is initiated up to 5 days post-challenge. High fever, viraemia and
abnormalities in blood count and blood chemistry were evident in many animals
before ZMapp intervention.
Advanced
disease,
as
indicated
by
elevated
liver
enzymes,
mucosal
haemorrhages and generalized petechia could be reversed, leading to full
recovery. ELISA and neutralizing antibody assays indicate that ZMapp is crossreactive with the Guinean variant of Ebola.
ZMapp exceeds the efficacy of any other therapeutics described so far, and results
warrant further development of this cocktail for clinical use
amiodarone
favipravir
Phase II trials in west Africa in the next 2-4 weeks
ChAd3-EBO-Z
(GSK Biologicals/NIAID)
chimpanzee adenovirus (ChAd3),
genetically engineered to express
gycoproteins from the Zaire specie
rVSV-ZEBOV
(NewLink/Merck)
vesicular stomatitis virus (VSV),
genetically engineered to express
gycoproteins from the Zaire specie
Liberia: 3 arms (ChAd3-EBO-Z; rVSV-ZEBOV; control vaccine): 9000x 3 pts
Guinea: ring design study
Sierra Leone: one vaccine with a stepped wedge approach
MALATTIA DA VIRUS EBOLA
DIREZIONE MEDICA
29-30-31 OTTOBRE 2014
Ci ricorderemo di loro dopo la epidemia?
1. Cuba :
2. Greece :
3. Monaco :
4. Belarus :
5. Austria
6. Georgia .
7. Italy :
8. Norway :
9. Switzerland :
10. ……..
11 ……..
640
604
581
487
475
454
424
408
407
http://www.worldmapper.org/display.php?selected=219
160. Guinea :
161. …..
10
186. Sierra Leone: 2
187. Liberia :
1
188. Tanzania :
1
A total of 820 health-care workers (HCWs) are known to have been
infected with EVD up to the end of 7 November: 154 in Guinea; 370
in Liberia; 11 in Nigeria; 296 in Sierra Leone; one in Spain; and three
in the United States of America (two were infected in the USA and
one in Guinea). A total of 488 HCWs have died (WHO; 7th Jan 2015)
http://www.indexmundi.com/map/?v=2226&l=it
Prof. Francesco Castelli
Chair of Infectious Diseases
UNESCO Chair
University of Brescia (Italy)
Harrison’s Principles of Internal Medicine, 18
18° edition, 2012
Chapers
Part 1. Introduction to clinical medicine
Part 2. Cardinal manifestations and presentations of diseases
Pages
Pages for ID
92
379
Part 3. Genes, the environment and diseases
40
Part 4. Regenerative medicine
20
Part 5. Aging
32
Part 6. Nutrition
58
12
Part 7. Oncology and hematology
361
11
Part 8. Infectious diseases
761
761
30
11
Part 9. Terrosism and clinical medicine
Part 10. Disorders of the cardiovascular system
286
Part 11. Disorders of the respiratory system
112
12
84
9
Part 13. Disorders of the kidney and urinary tract
122
9
Part 14. Disorders of the gastrointestinal system
248
23
Part 15. Disorders of the joints and adjacent tissues
216
7
Part 16. Endocrinology and metabolism
358
Part 17. Neurologic disorders
342
Part 18. Poisoning, drug overdose and evenomations
19
Part 12. Critical care medicine
3585
38
893 (24.9%)
Substantiated public health events of potential international
concern by hazard
Jan 2001-14 June 2011 (n=2,448; 477 (19%) in AMRO)
85%
Aldighieri, PAHO, 2012