I SESSIONE
Moderatori: G. Angarano, A. Di Leo
Pre e post-trapianto di fegato
nell’era dei nuovi antivirali
• Quali vantaggi dalle nuove terapie? N. Caporaso
• Stato dell’arte del paziente in lista d’attesa e del
paziente trapiantato M. Rendina
26 giugno 2014 Bari
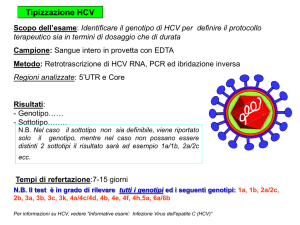
Primary Indications of Liver Transplantation
in 15936 Virus related Cirrhosis in Europe
01/1988 - 12/2008
Virus BC :
4%
Virus BCD :
145
1%
Other virus :
151
1%
Virus BD :
1198
8%
Virus B : 3893
24%
Virus C : 9859
62%
26 giugno 2014 Bari
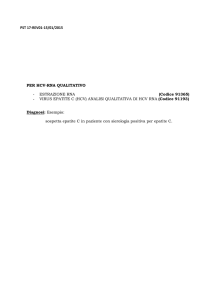
Survival of Patients with Virus related Cirrhosis as the
First Indication
01/1988 - 12/2008
(%)
(%)
100
94
90
81
81
80
83
75
82
69
71
67
65
66
60
60
58
54
40
20
0
0
1
2
3
Virus C : 9826
4
5
6
Virus BC : 688
7
8
9
Yrs
10
Virus BCD : 144
26 giugno 2014 Bari
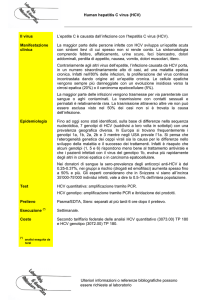
Accelerated Progression of HCV Disease
Following Liver Transplantation1,2
Nontransplant
Patients
Liver Transplant
Recipients
20% after 20 years
10%–40% after 5
years
• Cirrhosis to
decompensation
2.9%–3.7% per year
42% after 1 year
• Survival after
decompensation
50% after 5 years
50% at 1 year
30 years
10 years
• Chronic hepatitis to
cirrhosis
• Median duration to cirrhosis
1. Davis GL. Rev Gastroenterol Disord. 2004;4:7-17. 2. Rodriguez-Luna H, Douglas DD.
Curr Opin Infect Dis. 2004;17:363-371.
26 giugno 2014 Bari
The pre-transplant scenario: who
they are?
Pazienti CON C. HCV
SENZA
Cirrosi HCV
56%
CON
Cirrosi HCV
44%
Femmine
17%
Maschi
83%
•
Età media (±SD) al tx: 54 ± 8 anni
Percetuali calcolate sul totale dei pazienti valutabili con dato disponibile (N=1001).
26 giugno 2014 Bari
Punteggio MELD al tx in pazienti con
e senza cirrosi HCV
Pazienti SENZA C. HCV
Pazienti CON C. HCV
MELD <= 15
45%
MELD <= 15
49%
MELD > 15
51%
MELD > 15
55%
Analisi eseguite sul totale dei pazienti valutabili con cirrosi HCV (N=354) e senza cirrosi HCV (N=480).
26 giugno 2014 Bari
eGFR al tx in pazienti con e senza
cirrosi HCV
Pazienti SENZA C. HCV
Pazienti CON C. HCV
eGFR < 60
14%
eGFR >= 60
86%
eGFR < 60
17%
eGFR >= 60
83%
Analisi eseguite sul totale dei pazienti valutabili con dato disponibile con cirrosi HCV (N=379) e senza cirrosi HCV (N=495).
26 giugno 2014 Bari
26 giugno 2014 Bari
26 giugno 2014 Bari
26 giugno 2014 Bari
Goals of Antiviral Therapy in waitlisted
cirrhotic patients
• Halt or reverse disease progression
• Prevents allograft hepatitis
compensated
decompensated
26 giugno 2014 Bari
Outocome of antiviral therapy in HCV
decompensated cirrhosis
Author
Patients
Tx
EOT
SVR
Jacobellis
Forns
Tekin
Annichiarico
66
51
20
15
PEG/RBV
PEG/RBV
PEG/RBV
PEG/RBV
49%
29%
45%
47%
20%
20%
30%
20%
Everson
Forns
Thomas
Amarapurkar
Cripprin
Totals
124
30
20
18
15
391
IFN/RBV
IFN/RIBA
IFN
IFN/RBV
IFN/RBV
IFN/RBV
46%
30%
60%
61%
33%
44%
24%
20%
20%
38%
0%
23%
26 giugno 2014 Bari
Treatment discontinuation in cirrhotic patients during combination
therapy: safety warnings
278
Chronic hepatitis
87
Cirrhosis
85
Cirrhosis
66
Cirrhosis
90
Cirrhosis
Ishak score:
0 to 4
Ishak score:
5 or 6
portal hypertension
Decompensated
Child A, B, C
Decompensated
Chid A, B, C
40%
21%
16%
Infections
Side effects
6%
Floreani 2008
14%
11%
10%
Floreani 2008
Giannini 2009
Iacobellis 2007
Massoumi 2009
8%
Annichiarico 2008
26 giugno 2014 Bari
Cumulative incidence of bacterial infections
Carrion, J Hepatol 2009
26 giugno 2014 Bari
Pre-transplant SOF + RBV to prevent post-transplant
HCV recurrence
Post-transplant virologic
response rates
•
Listed for LT due to HCC meeting
Milan criteria
•
MELD exception for HCC
(mean MELD score = 8)
•
CTP score ≤7
•
Excluded decompensated cirrhosis,
renal impairment, living donor LT
Response (%)
Single-arm, open-label, Phase II study
from 16 LT sites
Pre-LT therapy: SOF 400 mg/day + RBV
1000–1200 mg/day for 48 weeks or until
time of LT
•
Post-LT immunosuppression:
≥12 weeks of tacrolimus +
prednisone + MMF
CTP = Child-Turcotte-Pugh; LLOQ = lower limit of quantification;
LT = liver transplant; MELD = model for end-stage liver disease;
MMF = mycophenolate mofetil; pTVR = post-transplant virologic response.
n
N
41
44*
25
39*†
* 3 subjects were >LLOQ at transplant.
† 1 subject has not reached pTVR12,
1 subject lost to follow-up at week 8
post-transplant.
Curry MP, et al. Hepatology 2013; 58 (Suppl 1):314–315A.
Pre-Liver Transplant Study (SOF+RBV)
Analysis of Post-Transplant Recurrence in GT 1–4
Days HCV RNA Continuously TND Prior to Transplant
No Recurrence (n=29)
Recurrence (n=10)
No recurrence in 24/25 (96%) of
patients who maintained HCV RNA
TND >28 days
Median days TND
• No recurrence: 99
• Recurrence: 5.5
p <0.001*
28
28
*Wilcoxon rank sum test.
Curry MP, et al. APASL 2014. Brisbane, Australia. Oral presentation
16
The transplant scenario
Author’s Last Name, Conference Name, Year, Presentation #
17
The interplay in the chimera scenario
Virus
Level of replication
Genotype
IL28………
Host
age, sex
fibrosis
comorbidities
………….
Chimera factors
donor (age, Il28b)
CNI
steroid boluses
CMV
immunologic imbalance
18
Baseline features of the Italian Recolt pts
464 HCV recurrent patients
treated with antiviral therapy
Median post-transplant follow up:
6.1 years (0.4-22.8)
HCV features
demography
Pre-LT therapy
Male
75%
ALT
31%
171±165
Recipient age 53±8yrs
Genotype 1-4
75%
BMI
25±3
High viral load
84%
Diabetes
50%
Grading
6.1±3
Staging
2.1±1.2
Facts about intererferon based therapy in Liver
transplant: applicability and safety
Mostly due to anemia
PEG-IFNα-2a
PEG-IFNα-2b + ribavirin
1. Chalasani N et al. Hepatology. 2005;41:289-298.
2. Rodriguez-Luna H et al. Transplantation. 2004;77:190-194.
3. Castells L et al. J Hepatol. 2005;43:53-59.
4. Dumortier J et al. J Hepatol. 2004;40:669-674.
Italian RECOLT-AISF cohort
Survival
1-yr
5-yrs
SVR
98.8±0.9%
87.2±3.0%
Non-SVR 92.0±1.6%
67.8±3.0%
Log-Rank p<0.001
Kaplan-Meier analysis of the cumulative survival from the start of therapy according
to the type of response to antiviral Therapy (SVR vs non-SVR). Survival was
significantly different in non-SVR compared with SVR patients (Log-rank test P<
0.001).
Rendina et al, Hepatol 2011
PI Triple Therapy in Liver transplant patients
Applicable to Genotype 1 only
More drugs------more side effects +++++anaemia
DRUG INTERACTIONS
Low effect in prior partial and NR to Peg+RIBA
22
SVR rates with triple therapy in Liver Transplant patients
50%
n = 273
n = 54
n = 95
n = 54
27/35
BOC
……………………………………
TVR
Wierner, Coilly, Puanpong, Stravitz, Nair 2013
23
Cmax increased by 9.3X
AUC Increased by 70X
Garg et al; Charlton M; Hepatol 201
24
Approach HCV eradication in transplant patients: a new era
SOF + RBV for treatment of post-LT HCV recurrence
Ongoing prospective, multicenter,
single-arm, open-label pilot study
SOF 400 mg/day + RBV
400–1200 mg/day for ≤24 weeks
Response (%)
• Median time since LT:
4.3 years (range: 1.02–10.6)
• CTP ≤7 and MELD ≤17
• 83% GT1, 33% IL28B CC,
40% with compensated cirrhosis
Virologic response rates
n
N
40
40
40
40
28
40
28
40
• RBV started at 400 mg/day
and increased based on
hemoglobin levels
Samuel D, et al. EASL 2014 [poster presentation 1232].
SOF + RBV ± PegIFN therapy: compassionate use program for
patients with severe HCV recurrence
Virologic response rates
100
Clinical outcomes
100
87.1
80
62.4
60
40
20
0
Patients (%)
Patients (%)
80
57.7
60
40
21.2
21.2
60
104
22
104
22
104
Improved*
Stable
20
n
N
81
93
53
85
EOT
SVR12
0
SOF 400mg/day for 24–48 weeks
+ RBV (± PegIFN) n=104
* Significant decrease in hepatic encephalopathy, improvement or
disappearance of ascites, or improvement in liver-related laboratory values.
n
N
Worsened/
deceased
All patients who received
>1 dose of SOF are included
Forns X, et al. EASL 2014 [oral presentation 62].
Sofosbuvir compassionate protocol in Italy
AISF sponsored SOFOLT Study
M. Rendina & P. Andreone coordinators
Start in April 2014
Preliminary data from 18 patients available from 7 centers on
April 30:
•
Bologna (R. Vukotic)
•
Pisa (P. Carrai)
•
Bari (A. Di Leo)
•
Parma (A. Degli Antoni)
•
Roma (L. Loiacono)
•
Roma (M. Merli)
•
AISF-SOFOLT study preliminary data
Genova (A. Picciotto)
27
Sofosbuvir compassionate protocol
Inclusion criteria
•
•
•
•
•
Age >18 yrs
Advanced liver disease (MELD ≥12; CTP ≥B7)
Life expectancy ≤6 mo
No access to experimental treatment
Stable immunosuppressive regimen
28
Sofosbuvir compassionate protocol
Exclusion criteria
•
•
•
•
•
Inability to sign informed consent
No advanced liver disease (CTP <B7)
Life expectancy >6 mo
Unstable immunosuppressive regimen
Pregnancy
29
Sofosbuvir compassionate protocol in Italy
Today status
87 patients received at least 1 dose of SOF
38 investigators involved
26 centers involved
4 different treatment schedules
•
•
•
•
SOF+RBV
SOF+SMV
SOF+DCV
SOF+RBV+Peg-IFN
3 different duration of treatment
• 12 wks
30
Results: Patient Disposition
Death
n=1
SOF + RBV for 24 wks
n=18
Completed 4 weeks
n=15
Completed 12 weeks
n=11
Completed 24 weeks
n=7
Completed 4 weeks FU
n=5
Completed 12 weeks FU
n=3
AISF-SOFOLT study preliminary data
31
Results: Baseline Characteristics
n=18
Forns, EASL 2014
n=104
Male, n (%)
13 (76.5)
76 (73)
Median age, y (range)
48 (25-56)
55 (16-76)
6.5 (1.3-7.3)
8.4 (1.3-8.9)
1a/1b
5/10
8/29/51
2/3/4
0/2/1
1/7/8
Median bilirubin, mg/dL (range)
3.3 (0.4-12)
3.1 (0.4-45)
Median albumin, g/dL (range)
3.4 (2.6-4.7)
3.1 (1.3-12.2)
Median INR (range)
1.3 (1-1.86)
1.3 (0.8-4.5)
Median platelets, x103/µL (range)
131 (7-871)
78 (19-340)
15 (5-26)
15 (6-43)
48 (0.6-168)
17 (1-262)
Median HCV RNA, log10 IU/mL (range)
GT, n
Median MELD (range)
Median months from LT to treatment, (range)
AISF-SOFOLT study preliminary data
32
Viral Kinetic
HCV-RNA UI/ml
baseline 4 wks
12 wks
24
wks
AISF-SOFOLT study preliminary data
33
Lab results (1)
BILIRUBIN mg/dl
baseline
4 wks
12 wks
24 wks
AISF-SOFOLT study preliminary data
34
Lab results (2)
ALBUMIN mg/dl
baseline
4 wks
12 wks
24 wks
AISF-SOFOLT study preliminary data
35
Lab results (4)
INR
baseline
4 wks
12 wks 24 wks
AISF-SOFOLT study preliminary data
36
Model for End Stage Liver Disease score
MELD score
baseline
4 wks
12 wks
24
wks
AISF-SOFOLT study preliminary data
37
Child Turcotte Pugh score
CTP score
baseline
4 wks
12 wks
24
wks
AISF-SOFOLT study preliminary data
38
Virological Response
AISF-SOFOLT study preliminary data
39
Interaction SOF/TAC
TACROLIMUS ng/ml
baseline
4 wks
12 wks
24
wks
AISF-SOFOLT study preliminary data
40
41
M12-999: ABT-450/RTV/Ombitasvir +
Dasabuvir + RBV in Transplant Recipients
•
•
•
Open-label phase II trial in liver transplant recipients with recurrent HCV GT1
Primary endpoint: SVR12
Inclusion criteria: GT1,naïve after transplant, METAVIR score
≤ F2, no previous steroid-resistant rejection, stable CNI-based
immunosuppressant regimen
Wk 24
Liver transplant recipients with
recurrent HCV GT1
(N = 34)
ABT-450/RTV/Ombitasvir + Dasabuvir + RBV
ABT-450/RTV/ombitasvir 150/100/25 mg once daily; dasabuvir 250 mg twice daily; RBV dosed at discretion of
treating physician.
Dosing of calcineurin inhibitors based on phase I PK study. Recommended tacrolimus dose modified to 0.5 mg once
wkly or 0.2 mg every 3 days. Recommended cyclosporine dose modified to 20% of daily dose administered before
study drugs. Prednisone ≤ 5 mg/day permitted. No use of mTOR inhibitors.
Kwo P, et al. EASL 2014. Abstract O114
Study M12-999: liver transplant recipients with recurrent HCV
GT1 infection – ongoing efficacy results
100
97.0
96.2
34
34
34
34
32
33
25
26
RVR
EOTR
SVR4
SVR12
(Week 4)
(Week 24)
Patients (%)
100
n
N
No patient experienced a viral breakthrough and one patient had a relapse (post-treatment day 3)
•
At the time of relapse, this patient had R155K in NS3 protease, M28T+Q30R in NS5A, and
G554S+G557R in NS5B, none of which were present at baseline
EOTR = end of treatment response.
Kwo P, et al. EASL 2014 [oral presentation 114].
Study M12-999: liver transplant recipients with recurrent HCV
GT1 infection – safety data
Adverse events in >15%
of patients, n (%)
Any AE
Headache
Fatigue
Cough
Insomnia
Asthenia
Diarrhea
Nausea
Rash
Anemia
Dizziness
Muscle spasms
Pyrexia
3D + RBV
(N=34)
33 (97.1)
15 (44.1)
14 (41.2)
10 (29.4)
9 (26.5)
8 (23.5)
8 (23.5)
8 (23.5)
7 (20.6)
6 (17.6)
6 (17.6)
6 (17.6)
6 (17.6)
No episodes of acute or chronic rejection
1 patient discontinued study drug due to
AEs (moderate rash, memory impairment,
and anxiety) after week 18
• Patient achieved SVR12
2 patients had serious AEs:
• Hypotension and tachycardia
associated with initiation of
tamsulosin (Flomax) after elective
surgery
• Moderate peripheral edema and
pain in extremity in a diabetic
patient with history of peripheral
edema
Kwo P, et al. EASL 2014 [oral presentation 114].
Open issues……..
- The potential of drug-drug interaction (CNI, HBV coinfection)
- Renal dysfunction
- Duration and doses
- Clinical impact of relapse
- Renal pts
- Resistance profile
26 giugno 2014 Bari
Decreto 8 maggio 2003 - Uso speciale dei
farmaci…cosi’ detto anche uso compassionevole
• normativa di riferimento che disciplina in Italia l’accesso
a terapie farmacologiche sperimentali, per un uso al di
fuori della sperimentazione clinica, a pazienti affetti da
malattie gravi o rare o che si trovino in pericolo di vita,
quando, a giudizio del medico, non vi siano ulteriori
valide alternative terapeutiche
• .
Decreto 8 maggio 2003 - Uso speciale dei
farmaci…cosi’ detto anche uso compassionevole
•
•
•
•
•
•
•
Richiesta del medicinale formulata dal medico con assunzione di
responsabilità al trattamento secondo protocollo ai sensi dell’art. 4
comma 2 lettera a) del DM 8/5/2003;
Notifica del/dei pazienti candidati al trattamento accompagnata da
breve motivazione clinica;
Protocollo d’uso del medicinale;
Documentazione di informazione al paziente accompagnata dal
modulo per l’acquisizione del consenso informato;
Dichiarazione di disponibilità della ditta alla fornitura del medicinale;
Parere espresso dal Comitato Etico;
Documentazione attestante la produzione del medicinale secondo
GMP in accordo alla normativa nazionale e comunitaria;