Agenti infettivi potenzialmente implicati in alterazioni a carico del fegato e delle
vie biliari
Virus
-HAV
-HBV
-HCV
-HDV
-HEV
Batteri
-Brucellae
-F.tularensis
* Primitivamente epatotropi
-Legionellae
-Leptospirae
-HGV
-SEN-V
-TTV
?
-Salmonellae
-C.burnetii
-Rickettsia spp.
-M.pneumoniae
-CMV
-EBV
-HSV-1, HHV-6
-VZV
-Coxsackievirus, Echovirus, Adenovirus, Parvovirus
-Virus della rosolia e della parotite
-Flaviviridae (v. della febbre gialla e v. della Dengue)
-Arenaviridae (v. della febbre di Lassa, v. Junin, v.
Machupo)
-Filoviridae (v. Ebola, v. Marburg)
-Bunyaviridae (v. della febbre della valle del Rift)
-E. coli, Enteobacter spp,
enterococchi, Klebsiella
spp, Proteus spp,
stafilococchi, anaerobi
Parassiti
-T.gondii
-Plasmodium malariae
-Strongyloides stercoralis
-Fasciola hepatica
-Clonorchis sinensis
-Opisthorchis felineus
-Opistorchis viverrini
-Dicrocoelium dendriticum
-Metorchis conjunctus
-Ascaris lumbridoides
-Echinococcus granulosus e
multilocularis
(Bacteroides fragilis,
Clostridium perfringens,
Fusobacterium spp)
…
Epatite
Lesione
necro-infiammatoria
del
parenchima
epatico
determinata
da
diversi
possibili
agenti
eziologici
infettivi e non
Epatiti virali da virus primitivamente epatotropi
Virus
Acido
nucleico
Famiglia
Genere
Trasmissione
Cronicizzazione
HAV
RNA
Picornaviridae
Heparnavirus
Fecale-orale
No
HBV
DNA
Hepadnaviridae
Orthohepadnavirus
Parenterale
Sì
HCV
RNA
Flaviviridae
Hepacivirus
Parenterale
Sì
HDV
RNA
Deltaviridae
Parenterale
Sì
HEV
RNA
Hepeviridae
Hepevirus
Fecale-orale
No*
*segnalati casi in ID
HAV
1,5 milioni di casi / anno
(… ma incidenza sottostimata)
1985: 10/100000
2006: 1,4/100000
-ubiquitaria, si distinguono forme sporadiche ed epidemiche
-alta prevalenza nei Paesi in via di sviluppo dove la malattia
interessa prevalentemente l’infanzia
-nei Paesi industrializzati viene interessata soprattutto l’età
adulta
-Italia: prevalenza di positività HAV-IgG dell’85% nella
popolazione adulta. 1985-1995: riduzione del tasso di
incidenza e della prevalenza tra i giovani, quindi aumento
della suscettibilità all’infezione
EPATITE A
Classificazione:
Famiglia Picornaviridae
Genere Heparnavirus
diametro 27-28 nm
simmetria icosaedrica
assenza di involucro
termostabile e resistente agli acidi
Genoma ad RNA lineare, a elica semplice,
di 7478 nucleotidi
HAV
è
caratterizzato
da
stabilità
antigenica (unico Ag – HA-Ag -, 4 genotipi,
ma 1 solo sierotipo)
In vitro, non ha effetto citopatico
(trasporto mediato da vescicole provviste di
membrana?)
In vivo, il virus potrebbe essere liberato
dalle membrane dai vari componenti della
bile, con la quale viene escreto dagli
epatociti
-Meccanismi di trasmissione:
fecale-orale +++
sessuale (> in omosessuali maschi)
parenterale (descritti casi in seguito a emotrasfusioni o in IVDA)
materno-fetale (molto rara)
-Serbatoio: soggetti sintomatici o asintomatici con infezione in atto
(non esiste lo stato di portatore cronico di HAV)
-Fattori di rischio:
Ingestione di acqua e cibi contaminati dalle feci di pazienti malati
(frutti di mare crudi, verdura e frutta crude, gelati, ghiaccio,
acqua….)
Viaggi in aree endemiche
Balneazione in acque contaminate
Contatti stretti con persone malate (conviventi, personale
sanitario…)
Rapporti sessuali anali-orali
PATOGENESI
Diffusione del virus nell’ambiente
attraverso le feci di pazienti malati
Ingestione
di
acqua
e
cibi
contaminati
Passaggio/replicazione attraverso
la mucosa intestinale (?)
Localizzazione
al
parenchima
epatico
Danno necro-infiammatorio
citopatico
diretto ?
CD8+
IFN-gamma
Escrezione biliare
Massiva presenza del virus nelle
feci
Viremia di lieve entità
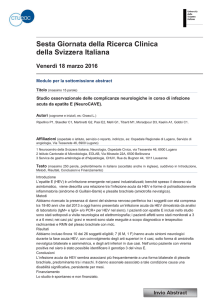
EVENTI IN CORSO DI INFEZIONE DA HAV
Fase sintomatica
Infezione
ALT
IgG
Risposta
IgM
Diagnosi
MARKERS SIEROLOGICI
Viremia
HAV-IgM: compaiono durante la fase acuta e
scompaiono dopo la guarigione.
Sono indice di infezione acuta
HAV-IgG: compaiono verso la fine della fase
acuta, restano positivi tutta la vita
e proteggono da future infezioni.
Sono indice di infezione pregressa
HAV nelle feci
0
1
2
3
4
5
6
7
Settimane
8
9
10
11
12
13
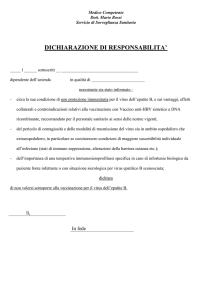
EPATITE A: decorso ed evoluzione
Periodo d’incubazione
15-50 giorni
Infezione
10-80%
Epatite Acuta
< 0,1%
100%
Guarigione Epatite fulminante
20-90%
Forme asintomatiche
0%
Cronicizzazione
- Incubazione: 15-50 giorni
-Decorso: in genere asintomatico (soprattutto nei bambini); nei casi sintomatici si distinguono
un periodo pre-itterico ad esordio improvviso con malessere, astenia, nausea, vomito, dolore
addominale superiore, un periodo itterico in genere preceduto da rialzo delle transaminasi
ed una fase di convalescenza
-Incidenza di epatite fulminante < 0.1% (> rischio per pz >40 aa o con epatite C cronica)
-Descritti alcuni casi a decorso protratto con andamento bi- poli- fasico delle transaminasi)
-Possibili ricadute a 2-5 sett. dall’esordio clinico di malattia
PROFILASSI
MIGLIORAMENTO DELLE CONDIZIONI IGIENICO SANITARIE
IMMUNOPROFILASSI PASSIVA
IG umane: somministrate pre- o post- esposizione, proteggono
dall’infezione per alcune settimane
IMMUNOPROFILASSI ATTIVA
Controindicazioni:
febbrili
acute,
Vaccino: costituito da virus vivo e attenuato m.
ipersensibilità alla 1°
Efficace in circa 100% casi
dose, gravidanza
Somministrazione i.m. in regione deltoidea
Schema vaccinale: 1°dose tempo 0; 2°dose dopo 6-12 mesi
Durata della protezione : 10-15 anni
Disponibile anche un vaccino associato anti-epatite A e B
(Twinrix)
Schema vaccinale: 1° dose tempo 0;
2° dose dopo 1 mese; 3° dose dopo 6 mesi
CHI VACCINARE ?
-Bambini* e adulti che viaggiano di frequente o per lunghi
soggiorni in aree a media/alta endemia
-Istituzionalizzati civili/militari
-Personale di asili infantili
-Omosessuali maschi
-Tossicodipendenti in aree endemiche/epidemiche
-Epatopatici cronici
-Candidati a trapianto d’organo
-Soggetti con malattie della coagulazione
-Addetti
alla
manipolazione/vendita
di
sostanze
alimentari
-Addetti agli impianti fognari e al trattamento delle acque
-Personale sanitario e di laboratorio
-Consumatori di molluschi eduli/pesce crudo
* In zone iperendemiche (> 20 casi su100000 ab.) a tutti i
bambini > 2 aa, >1 aa secondo indicazioni OMS e Ig sp. per
bambini < 1 aa non allattabili al seno
EPATITE E
Classificazione:
Famiglia Hepeviridae
Genere Hepevirus
-Struttura:
particella
sferica,
diametro 32-34 nm, assenza di
involucro
-Genoma: molecola di RNA a catena
singola, 7,5 Kb. Identificati 4
genotipi, 1 sierotipo
-Meccanismo
di
trasmissione:
fecale-orale (altre vie ipotizzate:
via
parenterale
classica
e
inapparente,
sessuale
e
verticale)
-Sorgente di infezione: acqua
contaminata (forse anche cibi)
Zoonosi ….
-Si distinguono una forma epidemica ed una
sporadica
-Il veicolo principale è l’acqua
-La trasmissione è fecale-orale
-Non c’è evidenza di trasmissione sessuale né
parenterale
Hepatitis E in high-income countries
Source
UMR 1161 Virology, AFSSA LERPAZ, ENVA, INRA. 23 Avenue du General de Gaulle,
94706 Maisons-Alfort cedex, France. [email protected]
Abstract
PURPOSE OF REVIEW:
To discuss recent advances in characterising viral Hepatitis E (HEV) in nonendemic
regions, with a special focus on epidemiology in high-income countries, different
clinical aspects of the disease, possible zoonotic origin of these cases and the
improvement of Hepatitis E diagnosis.
RECENT FINDINGS:
In high-income countries, most cases of Hepatitis E are acquired locally and not
imported from endemic regions. Different genotypes are involved in indigenous
cases than those in endemic regions. Particular population groups, such as
transplant recipients, can be persistently infected by hepatitis E and develop chronic
diseases. Viral hepatitis E is frequently observed in people in animal care
occupations. Indeed, HEV has a large animal reservoir and this emerging disease in
developed countries has probably a zoonotic origin.
SUMMARY:
Recent studies on viral Hepatitis E have shown that the epidemiology of the disease
differs between endemic and nonendemic regions. Several lines of evidence suggest
that Hepatitis E is more frequent than was suspected and that it has a possible
animal origin. Particular attention must be paid to the possible chronic evolution of
various forms of the disease. Surveillance of human cases and animal reservoirs must
be developed further.
Hepatitis E as zoonosis
Source
Zakład Epidemiologii Narodowego Instytutu Zdrowia Publicznego-Państwowego Zakładu
Higieny w Warszawie. [email protected]
Abstract
The hepatitis E virus (HEV) the causative agent of hepatitis E, is a non-enveloped RNA virus. HEV
is transmitted through oral consumption of contaminated food and water According to the
currently knowledge now be considered as zoonosis. The main reservoir of HEV are pigs, boars
and deer. For the first time HEV was isolated from animals (pigs) in 1997 in the U.S. Genetic
analysis of strains isolated from pigs showed high similarity to strains HEV isolated from
humans. This was the first evidence showing that HEV is a zoonosis. Further studies have shown
that occupational groups e.g. veterinarians, swine breeders with close contact to pigs have an
increased risk for HEV infections. The additional evidence supported the zoonotic potential of
HEV were reports of acute hepatitis E after the consumption of undercooked meat from deer and
wild boar. Infection of HEV in the domestic pig and wild boar population in Europe is
widespread.
Baumann Popczyka et al. Przegl Epidemiol. 2011;65(1):9-13.
A systematic review/meta-analysis of primary research investigating
swine, pork or pork products as a source of zoonotic hepatitis E virus
A significant association between occupational exposure to swine and
human HEV IgG seropositivity was reported in 10/13 cross-sectional
studies. The association reported between pork consumption and HEV
IgG seropositivity was inconsistent.
Wilhelm BJ et al. Epidemiol Infect. 2011 Aug;139(8):1127-44
Evidence of hepatitis E virus (HEV) infection in human and pigs in Sardinia, Italy
Source
Department of Public Health, University of Cagliari, Italy. [email protected]
Abstract
INTRODUCTION:
The aim of this study was to determine the seroprevalence of anti-HEV antibodies in humans
sera and to study HEV prevalence in swine from different Sardinian farms, testing viral HEVRNA in bile samples.
METHODS:
In the first six months of 2008, 532 subjects of whom 402 blood donors and 130 workers at
zoonotic risk, were enrolled. Anti-HEV were determined with an enzyme linked
immunosorbent assay (ELISA). In positive subjects, RNA was extracted and tested by RTNested-PCR. From July 2006 to March 2007, 95 bile samples were collected from randomly
selected pigs. RNA was extracted from 250 microl of bile and tested by RT-Nested-PCR.
RESULTS:
The overall prevalence of anti-HEV antibodies was 4.3%; 5.0% among blood donors and 2.3%
among workers at zoonotic risk, with no statistically significant differences between sex, age
classes and occupation. The search for HEV-RNA in the subjects positive for antibodies, gave
negative results. HEV genome was detected in 6 of the 95 swine bile samples tested.
Sequences were clustered within the genotype 3 and are edited on GenBank under accession
number: from FJ850960 to FJ850962 and from FJ883000 to FJ883002.
DISCUSSION:
The overall prevalence of anti-HEV shows that the virus circulates without giving origin to
cases of acute hepatitis. The low prevalence value found in workers at zoonotic risk do not
apparently support the hypothesis of professional risk. In this study, HEV-RNA was isolated
from pigs in Sardinia for the first time confirming the role of swine as HEV reservoir and the
possibility of virus transmission to humans.
Masia G. J Prev Med Hyg. 2009 Dec;50(4):227-31
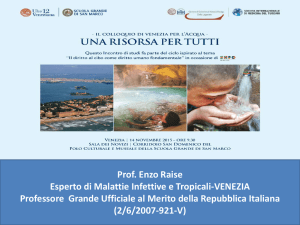
EVENTI IN CORSO DI EPATITE E
Titolo
Diagnosi
MARKERS SIEROLOGICI
SINTOMI
HEV-IgM: compaiono durante la
fase acuta e scompaiono dopo
la guarigione. Sono indice di
infezione acuta
HEV-IgG: compaiono nelle prime
settimane di malattia, in
genere dopo le IgM, e
persistono più a lungo, ma
probabilmente non per tutta
la vita (anticorpi protettivi?)
ALT
IgG anti-HEV
IgM anti-HEV
Virus nelle feci
0
1
2
3
4
5
6
Settimane
7
8
9
10 11
12 13
EPATITE E: decorso ed evoluzione
-Periodo d’incubazione: 2-9 settimane (40 giorni)
-Decorso: quasi sempre sintomatico; alla fase pre-itterica, di circa 10
gg, caratterizzata da esordio brusco con nausea, vomito e dolore in
ipocondrio dx, fa seguito la fase itterica; frequente la forma
colestatica
-L’andamento clinico è benigno, se colpisce, come di norma, i giovaniadulti
(15-40 aa)
-Quadri gravi se contratta in gravidanza (soprattutto nel III trim.)
Letalità del 25% o anche maggiore per insorgenza di encefalopatia,
diatesi emorragica, insufficienza renale …
Forme fulminanti: 1-12%
L’EPATITE E NON CRONICIZZA E NON ESISTE LACONDIZIONE
DI PORTATORE CRONICO DEL VIRUS …
Hepatitis E virus: an underdiagnosed cause of chronic
hepatitis in renal transplant recipients.
Source
Division of Nephrology, Cliniques Universitaires Saint-Luc,
Université Catholique de Louvain, Brussels, Belgium.
Abstract
Hepatitis E virus (HEV) infection can evolve to chronic
hepatitis in immunocompromised patients leading to rapidly
progressive cirrhosis. Proper diagnosis is therefore important,
as reducing immunosuppressive therapy can allow clearance
of the virus. We report a case of chronic HEV infection in a
renal transplant recipient that went undiagnosed for many
years, discuss the therapeutic options, and review the current
available literature.
Halleux D et al. Transpl Infect Dis. 2011
Chronic hepatitis E in an immunocompetent patient
Source
Servicio de Gastroenterología, Hospital Universitario Ramón y Cajal,
Madrid, España. [email protected]
Abstract
Hepatitis E virus (HEV) is a Hepevirus, with four different genotypes.
Genotypes 1 and 2 often cause acute hepatitis, which presents as
outbreaks in endemic regions of Asia and Africa. Genotypes 3 and 4
cause sporadic cases of acute hepatitis in Europe and North America,
where it is considered a zoonosis. Symptoms usually resolve
spontaneously, but in recent years cases have been detected that
progress to chronic liver disease mainly in immunocompromised
patients (patients with solid organ transplants, lymphoma, human
immunodeficiency virus, primary immunodeficiencies, and those under
treatment with corticosteroids and immunosuppressive agents..). We
report the case of a healthy, immunocompetent man who developed an
episode of acute HEV hepatitis, which progressed to chronic liver
disease with fibrosis grade III/IV in the liver biopsy within a year and
half.
Gastroenterol Hepatol. 2011;34(6):398-400
PROFILASSI
INEFFICACIA DELLA SOMMINISTRAZIONE DI IG UMANE O DI
FARMACI ANTIVIRALI DOPO ESPOSIZIONE ACCIDENTALE AL VIRUS
SOLO MONITORAGGIO PER DIAGNOSI PREOCE
ASSENZA DI VACCINO EFFICACE … in studio vaccini ricombinanti
PREVENZIONE IGIENICO-SANITARIA