Avian
Influenza
Massi Paola
Sezione di Forlì
IZSLER
Santa Sofia,26.10.2006
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Dal 2003 a giugno
2006 registrati
presso l’OMS 205
casi di infezione con
113 decessi
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• L’OIE segnala
focolai epizootici
negli uccelli
domestici e selvatici
in una cinquantina
di Paesi
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Per il 50% i casi di
contaminazione sono
stati registrati nei
soggetti con meno di
20 anni, il 90%in
quelli con meno di 40
anni
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Quanto ai bambini
colpiti
dall’infezione, 21
avevano meno di 5
anni e 32 tra 5 e 9
anni.
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Il fatto che la maggior
parte dei casi
interessa soggetti di
età compresa tra i 10
e i 29 anni potrebbe
spiegare la loro
presenza nei Paesi
dove la popolazione è
giovane
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Per esempio, Egitto e
Indonesia, nel 2005,
dove rispettivamente il
34 e il 28% della
popolazione ha meno
di 15 anni.
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Inoltre, i comportamenti legati
all’età o al sesso (es.lo
spiumaggio,la macellazione e
la preparazione degli alimenti
vengono effettuati dalle
giovani donne e i bambini
giocano con volatili infetti)
aumentano il rischio di
esposizione prolungata e di
stretto contatto con i volatili
infetti.
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Tuttavia, nessuna
differenza
statisticamente
significativa è stata
evidenziata fra gli
uomini e le donne
quanto al rischio
dell’infezione
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Il livello generale di mortalità si assesta al
56%.E’ elevato per tutte le età anche se
raggiunge il 73% dai 10 ai 39 anni
• Il livello più basso (18%) si registra negli over
50.
• Il livello di letalità differisce da quello
dell’influenza stagionale”tradizionale”per la
quale la mortalità più elevata si registra nelle
persone più anziane.
La letalità media del virus dell’influenza aviaria
H5N1 (OMS)
• Il livello generale più elevato di mortalità si è
raggiunto nel 2004 con il 73%
• Durante gli ultimi tre anni, l’incidenza di
mortalità ha raggiunto il picco nel corso del
periodo inverno-primavera dell’emisfero nord
DIAGNOSIS
• Clinical, gross amd microscopic findings
• Laboratory diagnosis
Meat-type and breeder turkeys
Before 1999
• We known H6 and H9 in turkeys
• Respiratory signs
• Inactivated vaccines
H7N1 LPAI
1999 Year
Low pathogenicity avian influenza (LPAI)
Clinical findings
• Mortality rates ranging from 5 to 97%
• Depending of the age, on a series of
environmental factors
(temperature,ventilation,hygienic conditions)
and the presence of infectious agents
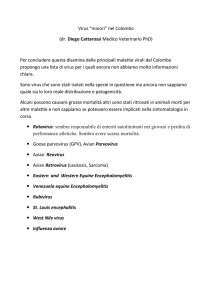
Low pathogenicity avian influenza (LPAI)
• During the fase acute of
the disease,
depression,ruffled feathers
and congiuntivitis
• Swelling of infraorbital
sinuses with caseous clots
• Egg production dropped
from 30 to 80%
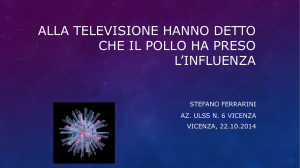
Swelling of infraorbital sinuses
Low pathogenicity avian influenza (LPAI
• Swelling of
infraorbital sinuses
with caseous clots
Low pathogenicity avian influenza (LPAI
Haemorrhagic tracheitis
Lungs congested and haemorragic
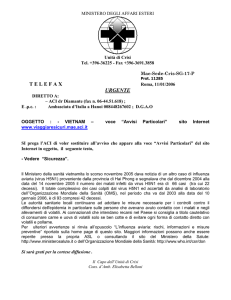
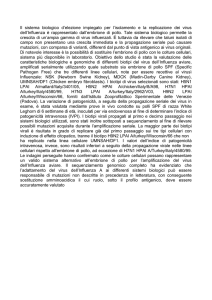
H7N1 HPAI
2000 Year
Severe depression in preagonic phase and dead birds on their back
due
to nervous signs and spastic contractions prior to death
Highly pathogenic avian influenza (HPAI)
• In meat-type and breeder turkeys, 100% mortality 4872 hours from the onset of the first clinical signs.
• Drop in food consumption and nervous signs
Highly pathogenic avian influenza (HPAI)
• Post mortem findings
Haemorrhagic tracheitis with caseus clots
Pancreatitis and duodenitis
Necrosis of pancreas
Haemorrhages on the caecal tonsils
Polmonite acuta
Chicken
LPAI
Broilers and broilers breeders
Clinical findings
• In the majority of flocks, LPAI did not cause any
clinical signs
• In a limited number of outbreaks was characterised
by anorexia and mild respiratory signs, with low
mortality, in the order of 2-3%
LPAI
• Post mortem findings
• Polmonary and tracheal congestion with
cattarrhal tracheitis
• Ovarian follicles haemorrhagic and
oedematous
LPAI
Caged layers
Clinical findings
• Only 10-20%of the birds with loss of appetite and
depression, with very mild respiratory signs and
congestion of combs
• Drop in egg from 2 to 10% until 30%
• Mortality between 0.5 and 2%
LPAI
• Post mortem findings
• The lungs and tracheas were congested
• The ovary and oviduct edematous and
haemorrhagic
Lungs and trachea congested
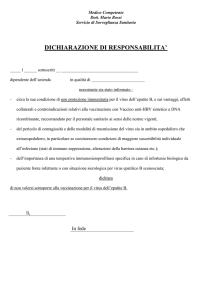
HPAI
• Chickens reared on litter
• Clinical findings
• 100% mortality 48-96 h.from the onset of the
first clinical signs
• Anorexia, depression and cessation of egglaying were followed by complete reluctance
to move and tremors of the head and
paralysis of the wing and legs
HPAI
• Caged layers
• Clinical findings
• The disease moved more slowly within the
flock
• Sonnolence, cessation of egg-laying and
feed consumption.
• Cianotic coombs with tremors of the head
HPAI
• Post-mortem findings
• Pancreatitis, caecal tonsils haemorrhagic
• Internal organs appeared congested
• Urate deposits in the kidney
Duck and goose
HPAI
Clinical findings
• Incoordination and tremors and mortality 5060%
Post mortem findings
• Pancreatic lesions
• Heart congested
• Duodenum congested
Japanese quail
(coturnix coturnix japonica)
HPAI
• Severe respiratory condition, prostration and
diarrhoa
• Nervous signs with torticollis and
opistothonus
• High mortality
Ostrich
(struthio camelus)
Ostrich
(struthio camelus)
• Clinical signs were observed only in juvenile
(7-9 months of age)
• anorexia, depression
• Feed consuption dropped
• Nervous signs
• haemorrhagic faeces
• Mortality 1-20%
H7N3
LHAI
2002 year
Laboratory diagnosis
A presumptive diagnosis can be made by
• Detecting antibodies
A definitive diagnosis of AI is established
by:
1. Direct detection of AI viral proteins or
genes in specimens such as tissues, swab,
cellculture or embryonating eggs
2. Isolation and identification of AI virus
Sample selection and storage
• Tracheal and cloacal
swabs or tissues
collected
• If the samples can be
tested within 48h. After
collection they may be
kept at 4°C; if over 48-72
h., storage at -70°C
Direct detection of AI viral protein or
Nucleic acid
•
Antigen capture ELISA
to detect viral antigens
in samples
Elisa sandwich virologica
Con Mab anti NPA (HB65)
Direct detection of AI viral protein or
Nucleic acid
• a human influenza test (Directigen BectonDickinsos) used to detect influenza viral
antigen
• This antigen capture enzyme immunoassay
was found to be specific and sensitive in
tracheal swabs
KIT IMMUNOENZIMATICO
Kit immunoenzimatico
Tamponi ed estratti d’organo per kit rapido
Commercial Rapid Ag Tests
•
•
•
• Advantages
1. Rapid
2. User-friendly
3. On farm test
•
•
• Disadvantages
1. Very high cost
2. Poor sensitivity
Direct detection of AI viral protein or
Nucleic acid
• Polymerase chain reaction
methods used are more
sensitive than virus
isolation procedures
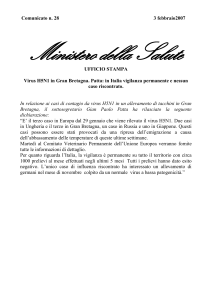
RT-PCR
M
ctrl+
1
2
3
4 Ctrl-
H7
H5
M
H5+
H7+
Metodo identificativo del genoma virale
PCR-Real Time
Quantitative real time PCR
Allows detection of the amplicon as it
accumulates by measuring light emission via a
specific probe. This light emission is linked to
amplicon production
PCR
•
Advantages
Sensitivity/ specifity
Rapid test
• Disadvantages
• High cost
Virus isolation
• Chicken embryos,10-11
days old,inoculated via
the allantoic cavity
Virus isolation
• The presence of virus is
demostrated by chicken
erythrocyte
haemagglutinating
activity (HA) in the
allantoic fluid
Virus isolation
• Plaque assay on cell
monolayers (MDCK)
MDCK
Madin Darby Canine
Kidney Cells
Virus identification
• 1) H.I. assay against NDV
and other paramixo
Virus identification
• 2) Double
immunodiffusion test
AGP to dectect the typespecific NP and matrix
proteins
Virus identification
• 3) ELISA with monoclonal
antibodies reacts with the
nucleoprotein or matrix
proteins
Virus identification
• 4) The next spet is to
determine the antigenic
subtype of the surface
antigens: HA and NA
• The HA is identified in the HI
test using a panel of antisera
prepared against the distinct
HAs
VIRUS ISOLATION
•
Disadvantages
No rapid
Cost
•
Advantages
• Virus isolation is important
for patogenicity studies
Serology
Specific antibodies detect as earlyas
seven days after infection
Serology
• In serological surveillance
programs:
• A) AGP test is used for the
detection of anti-NP antibodies
• Group specific
Serology
• B) ELISA assays
have been
developed to detect
antibodies AI virus
Serology
• C ) Once influenza is detected by AGP or
ELISA, HI test and ELISA with Mabs can
be used to determine the HA subtype
• Subtype specific
Paolo Cordioli