caricato da
hackertunel1
Chemotherapy Infusion Risks: A Nursing CPD Article

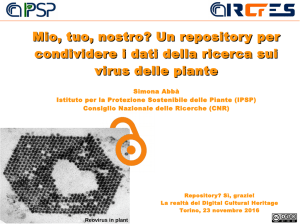
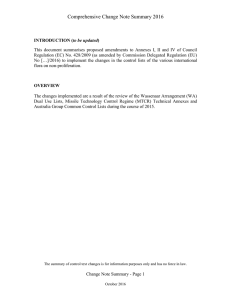
CPD CONTINUING PROFESSIONAL DEVELOPMENT Infusion-related risks associated with chemotherapy NS831 Gallimore E (2016) Infusion-related risks associated with chemotherapy. Nursing Standard. 30, 25, 51-58. Date of submission: May 29 2015; date of acceptance: October 7 2015. Aims and intended learning outcomes Abstract This article provides a comprehensive overview of the risks associated with the administration of chemotherapy, monoclonal antibodies and targeted or biological therapies in the management of solid tumours. The main physiological actions of these agents are discussed, with reference to the immediate infusion-related side effects and complications that may arise from an extravasation injury. The article focuses on the identification and early recognition of these risk factors to implement preventive measures and appropriate management strategies. Author Elizabeth Gallimore Oncology research practitioner, Clatterbridge Cancer Centre, Merseyside, England. Correspondence to: [email protected] Keywords biological therapies, chemotherapy, extravasation, infusion reactions, monoclonal antibodies, oncology, side effects This article aims to improve nurses’ knowledge of the infusion-related risks of chemotherapy and targeted therapies for solid tumours. After reading this article and completing the time out activities you should be able to: Describe the physiological action of chemotherapy, monoclonal antibodies and targeted therapies. Recognise infusion-related risks and side effects of chemotherapy and targeted therapies. Identify management strategies to reduce the risk of infusion-related side effects and complications. Outline the implications of early recognition and medical management of infusion-related risks. Review Introduction All articles are subject to external double-blind peer review and checked for plagiarism using automated software. Kang and Saif (2007) stated that ‘infusion related reactions may be defined as any signs or symptoms experienced by a patient during the infusion of pharmacologic or biologic agents or any event occurring on the first day of drug administration.’ Zetka (2012) suggested that all systemic anticancer therapies, whether chemotherapy, monoclonal antibodies or novel agents, have the potential to cause an infusion-related reaction. It is essential to develop an understanding of the presenting symptoms and management strategies to promote early recognition and prompt medical intervention to minimise complications. Certain classes of chemotherapy have a greater potential to cause an infusion-related reaction; these, in addition to the associated risks with monoclonal antibodies, are discussed in more detail. Complete time out activity 1 Revalidation Prepare for revalidation: read this CPD article, answer the questionnaire and write a reflective account. www.rcni.com/revalidation Online For related articles visit the archive and search using the keywords above. To write a CPD article: please email [email protected] Guidelines on writing for publication are available at: journals.rcni.com/r/author-guidelines. NURSING 17 other :: voluses 30 no 25 ::permission. 2016 51 DownloadedSTANDARD from RCNi.com by ${individualUser.displayName} on Aug 08, 2016. For personal february use only. No without Copyright © 2016 RCNi Ltd. All rights reserved. CPD oncology Anticancer therapies To fully appreciate the implications of chemotherapy and targeted therapies, including monoclonal antibodies, it is important to define the action of these agents and the physiological effect they have on the cells, paying particular attention to the mechanisms involved in infusion reactions and extravasation injury. Chemotherapy 1 Reflect on your own practice. List the most common complications you have experienced when managing patients undergoing chemotherapy. The term chemotherapy encompasses a range of different cytotoxic agents used to target and destroy cancer cells. Some cytotoxic anticancer drugs may not have the potential to cause cell death through their mechanism of action; however, they have the ability to induce mutations in the cancer cells. This allows detection by the immune system, which in turn triggers the physiological response of apoptosis. Chemotherapy acts to limit tumour growth and cause cell death through the activation of apoptosis and the inhibition of mitosis and proliferation. However, it does not target other aspects of tumour progression, including tissue invasion, angiogenesis, metastases or loss of differentiation. This means that, although cellular growth may be contained, the chemotherapeutic agents do not destroy those cells that have already migrated outside the primary tumour (Payne and Miles 2008). A consequence, or rather a complication, of chemotherapy regimens is the development of resistance to chemotherapy. Resistance occurs as a result of a cellular response to drug exposure that limits the efficacy and effectiveness of chemotherapy, leading to tumour growth and disease progression (Gatti and Zunino 2005). Dual therapy with two cytotoxic agents is often used to target high numbers of cancer cells and may be used in conjunction with other targeted therapies such as hormonal treatments or monoclonal antibodies, in addition to surgical intervention and the use of radiotherapy. However, this largely depends on the type of cancer, the rate of growth of cancer cells, and the aims and implications of treatment. Combination regimens may also help to delay the incidence of resistance to chemotherapeutic agents (Malhotra and Perry 2003). Chemotherapy can be highly successful, depending on several factors, including the extent of the disease, nature of treatment, presence of comorbidities and overall health status of the patient. Chemotherapy is not able to distinguish between healthy cells and cancerous cells and therefore attacks both, causing a number of side effects, including bone marrow suppression, which can have potentially fatal consequences. Both healthy and cancerous cells with a high growth rate are more sensitive to the actions of chemotherapy; patients may experience side effects owing to the damage to healthy cells as a result of the cytotoxic agents, including cells in the gastrointestinal tract, leading to mucositis, nausea, vomiting, bowel complications, damage to the hair follicles and, more importantly, the bone marrow as mentioned above. The distinguishing characteristic of this process is the ability of healthy cells to repair themselves and regenerate, whereas the cancer cells die if they are unable to replicate (Payne and Miles 2008). The presence of comorbidities can have a significant effect on whether the patient is likely to tolerate the toxicities of chemotherapy. Older people are compromised as a result of age-related physiological changes that affect their ability to tolerate the cytotoxic effects on the body, in addition to the associated complications of any concomitant medications and coexisting medical problems (Repetto 2003). The different classes of chemotherapeutic agents are not discussed in detail in this article. Certain risk factors and toxicities may be more prevalent depending on which cytotoxic agent is used; the reader should refer to their local policies and guidelines on the administration of chemotherapy to ensure safe and effective practice. Platinum-based compounds and taxanes are the two most common cytotoxic agents associated with infusion-related reactions. Targeted and biological therapies The aim of this article is to discuss the principles of infusion-related reactions linked to the administration of chemotherapy agents. However, it is important to mention that other targeted and novel therapies also have the potential to cause infusion-related reactions. These agents are becoming more widely used in conjunction with chemotherapy as a result of their milder toxicity profiles and additional potential benefits (Gerber 2008). It is beyond the scope of this article to discuss each targeted therapy in detail; however, reference is made to ensure that the reader develops an understanding of the potential risks of administering these products. 52 february 17 ::from vol RCNi.com 30 no 25 by :: 2016 STANDARD Downloaded ${individualUser.displayName} on Aug 08, 2016. For personal use only. NoNURSING other uses without permission. Copyright © 2016 RCNi Ltd. All rights reserved. Targeted therapies and biological agents act on specific molecules to inhibit tumour growth and progression, and the spread of cancerous cells. A broad range of targeted therapies have been developed to work in conjunction with chemotherapy agents and form treatment pathways for several different tumour groups. Transduction inhibitors target epidermal growth factor receptors and tyrosine kinase enzymes to prevent tumour progression and growth. Other targeted therapies focus on hormones, gene expression modulators, apoptosis inducers and angiogenesis inhibitors that target vascular endothelial growth factors. Immunotherapies and monoclonal antibodies may trigger the immune system to attack and kill the cancer cells, or they may attach themselves to the cancer cells to make them more visible to the immune system. The action of these agents depends on their specific pharmacodynamics; they have the ability to block specific signalling pathways that prevent the growth of cancer cells (Gerber 2008). Any pharmacological or biological agent has the potential to cause an infusion-related reaction, but there are clear documented risks with specific agents. Among targeted therapies, monoclonal antibodies in particular carry an increased risk of infusion-related reaction that is similar to a taxane response (Chung 2008). Monoclonal antibodies are classified as targeted therapies that have the ability to recognise and attach to certain proteins on the cancer cells. Each monoclonal antibody has a specific mechanism of action that depends on the cellular protein it is designed to target; these agents differ depending on the tumour and type of cancer. Monoclonal antibodies encompass a wide range of agents, including cetuximab, rituximab, trastuzumab, bevacizumab and panitunumab (Chung 2008). It is also important to make reference to novel therapies administered in a clinical trial setting. These agents, especially in early phase studies, do not have a fully developed safety profile, so a high index of suspicion is required when monitoring for infusion-related reactions. It is essential to be aware of the specific infusion reaction management strategies for each agent as set out in the study protocol, as well as any additional safety concerns, to appropriately treat any complications that arise. Complete time out activity 2 Infusion reactions One of the most prominent risks associated with the administration of systemic anticancer therapy is the possibility of an allergic reaction. The mechanisms involved in an immune-related response to both chemotherapy agents and targeted therapy can be treatment specific and depend on the class of agent used (Castells and Matulonis 2015). During initial exposure, immunoglobulin E (IgE) antibodies are produced and bind to the mast cells and basophils of the immune system. As the infusion progresses, or on subsequent infusions, the antibodies react to the antigen and cause a hypersensitivity reaction, resulting in the release of histamines, leukotrienes and prostaglandins from mast cells in tissue and basophils in peripheral blood. These reactions are characterised by the contraction of smooth muscle and dilation of the peripheral vessels. The exact physiology of chemotherapy-related reactions is unknown; some reactions occur as a result of a direct effect on the immune cells, while others may occur as a result of an anaphylactoid response through direct interaction with mast cells and basophils (Lenz 2007). Collectively, the occurrence of an allergic or hypersensitive reaction is the response of the immune system to a cytotoxic or biological agent considered a foreign protein. Reactions are most commonly mild, but they may develop into severe life-threatening complications without prompt recognition and implementation of management strategies (Vogel 2010). The symptoms of an infusion-related reaction to chemotherapy are largely dependent on the severity of the reaction and can be agent specific. Presenting symptoms include facial flushing, nausea, urticarial rash, back pain, chest pain, shortness of breath resulting from angioedema and bronchospasm, hypotension, tachycardia, drowsiness and episodes of syncope (Gottlieb et al 2010). When administering chemotherapy and monoclonal antibodies, it is essential to have an understanding of the risk factors associated with that particular drug to acknowledge whether an infusion-related reaction is likely to occur. As previously mentioned, taxanes and platinum-based compounds have the greatest potential to cause infusion-related reactions; however, the physiology differs somewhat between these two classes. Taxanes have the potential to cause a reaction as a result of the immediate effect of the biological agent on the immune cells. Precautions are taken in the form of 2 Reflect on the mechanism of action of chemotherapy agents and write brief notes on the following: How do they work? What effect do they have on the cancer cells? What is the rationale behind the side effects? NURSING 17 other :: vol uses 30 no 25 :: permission. 2016 53 DownloadedSTANDARD from RCNi.com by ${individualUser.displayName} on Aug 08, 2016. For personal february use only. No without Copyright © 2016 RCNi Ltd. All rights reserved. CPD oncology premedication to pre-empt and prevent a reaction. Agents such as docetaxel and paclitaxel pose a significant risk of allergic reactions (Vogel 2010), and prophylactic corticosteroids and antihistamines are used to reduce this risk. The use of premedication does not remove the risk of an infusion-related reaction, but does help to minimise the risk (Gottlieb et al 2010). The value of premedication may significantly decrease with further infusions of taxane agents, since the risk of an infusion-related reaction decreases with subsequent infusions (Chung 2008). Most infusion-related reactions occur within ten to 30 minutes of the initial or second administration. Evidence suggests that most reactions occur as a result of a direct effect on the immune cells and may be classified as an anaphylactoid response (Lenz 2007). In the case of monoclonal antibodies, the physiology behind an infusion-related reaction is not clearly understood, but has been strongly linked to the mechanisms involved in a reaction to taxane chemotherapy agents; premedication may also be used in the administration of monoclonal antibodies. Monoclonal antibodies interact with their molecular targets on the tumour cells and blood cells at the tumour site, resulting in the release of cytokines. Cytokines are hormone-like proteins that elicit an immune response, leading to the symptoms associated with a systemic infusion reaction (Pérez Fidalgo 2012). The presenting symptoms of a reaction to a monoclonal antibody are similar to a chemotherapy reaction, with a higher prevalence of skin involvement in the form of pruritus, rash and urticaria (Lenz 2007). In contrast, certain other cytotoxic agents – particularly platinum-based regimens with drugs including carboplatin, cisplatin or oxaliplatin – exhibit a classic IgE response. This response is also seen with the monoclonal antibody rituximab. These medications elicit a standard IgE response, with a reaction likely to occur after administration of multiple cycles, suggesting previous sensitisation (Kang and Saif 2007). Management strategies It is important to be aware of the potential for a reaction to take place and to have the knowledge, resources and ability to administer remedial therapy should a reaction occur. It is essential to be familiar with local policies on anaphylaxis and to have a good understanding of the principles of management strategies (Vogel 2010). Most chemotherapy units have an anaphylaxis kit to manage such situations. Standard treatment of a chemotherapy-related reaction is based on the administration of remedial drug therapy. The use of hydrocortisone and an antihistamine, usually chlorphenamine maleate, to control and reverse the immune response is highly effective, but adrenaline (epinephrine) may be required. The reader should refer to their local guidelines on managing anaphylaxis. Vogel (2010) provides a comprehensive algorithm for the management of a hypersensitivity reaction. The immediate response to a reaction is to stop the chemotherapy and commence a 0.9% sodium chloride infusion to prevent any further chemotherapy from being administered. A fast-flowing infusion of 0.9% sodium chloride should be administered to ensure haemodynamic stability and to aid in the administration of remedial drugs into the bloodstream. The patient’s vital signs should be monitored closely for any clinical deterioration, and a full clinical assessment should be performed. High-flow oxygen therapy is likely to be administered to assist in the treatment of the allergic reaction, but it should be noted that some chemotherapy agents may be associated with additional adverse reactions to the use of oxygen. Oxaliplatin, for example, is sensitive to cold air and may result in laryngeal spasms in the event of oxygen administration, leading to further complications and a potentially dangerous situation for the patient (Castells and Matulonis 2015). Preventive strategies should be in place to reduce the risk of laryngeal spasm. Avoiding cold food and drinks, wrapping up warm and slowing down the rate of administration of responsible agents may all help to reduce the incidence of this complication. If laryngeal spasm should occur, it is important to keep the patient calm, apply a warm compress to the area of the throat and encourage the patient to sip a warm drink if they are able. In severe cases, more definitive measures may be required. Allergic reactions are unpredictable and may not respond to treatment, so close observation, readiness to act and a comprehensive algorithm are essential. Patient education is another important factor in the prevention and management of these reactions. Educating the patient on the side effects and risk factors associated with their treatment emphasises the importance of early recognition of infusion-related reactions (Castells et al 2008). As mentioned, certain medications, such as paclitaxel or docetaxel, pose a significant risk within minutes of the 54 february 17 from :: vol RCNi.com 30 no 25 by :: 2016 STANDARD Downloaded ${individualUser.displayName} on Aug 08, 2016. For personal use only. NoNURSING other uses without permission. Copyright © 2016 RCNi Ltd. All rights reserved. first infusion, while others may present a problem further along the treatment schedule. Platinum-based therapies such as carboplatin and cisplatin may cause an allergic reaction after six cycles, which can be quite severe and difficult to treat. Patients receiving multiple doses of chemotherapy may become sensitised to the drug, and subsequent exposure may result in a hypersensitivity reaction (Castells et al 2008). Education, close monitoring, early recognition and a rapid response according to a documented treatment algorithm with best practice guidelines should be at the forefront of nursing practice in relation to infusion-related reactions to chemotherapy. It is important to document the incidence and severity of an allergic reaction accurately to provide a detailed account. Incomplete documentation or false representation of the severity of the reaction may affect the patient’s chance of being offered a re-challenge with the same drug or similar classes of drugs, thus limiting their treatment options. Safety concerns may be raised about the use of subsequent infusions, and additional precautions may be taken to minimise further risk (Vogel 2010). The decision to re-challenge depends on the aetiology of the severe reaction and an understanding of the mechanism of the individual agent. A re-challenge is the re-administration of a cytotoxic agent that previously caused an infusion reaction, usually at a slower rate of administration with the aid of premedication, to promote desensitisation. The aim of a re-challenge is to allow for treatment administration of those chemotherapeutic agents which cause an initial reaction but may be tolerated with subsequent infusions. Complete time out activity 3 Extravasation injury Extravasation refers to the inadvertent infiltration of cytotoxic agents into the extravascular space and surrounding tissues. Extravasation of targeted therapies does not pose the same risk as chemotherapeutic agents; the damage and potential for injury is significantly increased with cytotoxic medication. However, it is still important in this setting to be aware of an extravasation risk and the resulting complications (Pérez Fidalgo et al 2012). Misplacement of a peripheral cannula, poor selection of venous access and accidental damage to a cannula through movement may cause an extravasation injury (Pérez Fidalgo et al 2012). Chemotherapy agents are classified by their potential to cause damage should an extravasation injury occur and may be subdivided into three categories: Vesicant. Irritant. Non-vesicant. Owing to their toxic nature, vesicant chemotherapy drugs have the potential to cause the most damage. A high index of suspicion should be adopted when treating patients with these drugs; first to assess for risk factors and then to monitor actively for signs and symptoms of an extravasation injury to ensure prompt identification and implementation of management strategies to limit damage. Many, but not all, extravasation injuries can be prevented through a thorough risk assessment and the ‘systemic implementation of careful, standardized, evidence-based administration techniques’ (Pérez Fidalgo et al 2012). The insertion of a peripherally inserted central catheter (PICC) can significantly reduce the risk of an extravasation injury; it is recommended and is hospital policy in certain organisations for the administration of vesicant chemotherapy agents. An extravasation injury may still occur with a PICC, but the risks are very low with correct management and monitoring techniques (Schulmeister 2010). Box 1 lists the risk factors associated with an increased incidence of extravasation injury; it should be noted that this is not an exhaustive list. 3 Reflect on your experience of an infusion-related reaction. What were the main management strategies? Locate the clinical guidance for the management of infusion-related reactions in your practice area. Locate the anaphylaxis kit and familiarise yourself with its contents. BOX 1 Risk factors associated with extravasation injury Poor venous selection – small fragile veins or hard sclerosed veins. Poor site selection – an area that makes it difficult to detect the incidence of an extravasation injury; previous multiple cannulation attempts, including damage that occurred during previous treatment cycles. Poor insertion and management techniques and failure to adequately assess patency – the use of inappropriate or inadequate equipment for the task and fixation of the cannula once inserted may significantly increase the risk of an extravasation injury. Untrained or inexperienced staff. Patient-associated factors – including obesity, history of comorbidities such as peripheral vascular disease or diabetes, and the presence of lymphoedema – that make the process of inserting a cannula more difficult. Lack of patient education regarding the implications of extravasation injuries and difficulties in communication. Medical problems associated with altered peripheral sensation that can impair the patient’s ability to recognise symptoms. Prolonged infusions, especially of vesicant and irritant agents. High flow pressure and the administration of bolus medication. (Adapted from Pérez Fidalgo et al 2012) NURSING 17 other :: vol uses 30 no 25 :: permission. 2016 55 DownloadedSTANDARD from RCNi.com by ${individualUser.displayName} on Aug 08, 2016. For personal february use only. No without Copyright © 2016 RCNi Ltd. All rights reserved. CPD oncology 4 Define extravasation and list three known risk factors. Locate the extravasation policy in your area and become familiar with the guidelines. Choose one chemotherapy agent and research the extravasation management of that particular agent. The degree of damage depends on the type and concentration of chemotherapy, the length of time the drug has leaked into the tissues and the localisation of the area of extravasation. For example, a vesicant chemotherapy such as epirubicin given via a peripheral cannula in the hand has the potential for severe damage as a result of the toxicity of the drug and the implications for the surrounding area should an extravasation occur (Pérez Fidalgo et al 2012). Table 1 gives an overview of the different classes of cytotoxic drugs and their potential to cause an extravasation injury, making reference to the most commonly used chemotherapeutic agents. It should be noted that this is not an exhaustive list. Prompt recognition is essential to prevent severe damage to the tissues and peripheries surrounding the cannulation site. An extravasation injury has the potential to cause tissue necrosis, functional impairment and permanent disfigurement if left untreated. Surgical intervention may be required, depending on the severity of the injury, which may in turn result in a delay in planned chemotherapy treatment with complications lasting many months (Schulmeister 2010). TABLE 1 Potential for extravasation injury associated with cytotoxic drugs Class of agent Potential for injury Examples of agents Vesicants Capable of causing pain, inflammation and blistering of the local skin and underlying structures. Extravasation of this agent can result in tissue death and necrosis. Epirubicin, doxorubicin, mitomycin, dacarbazine, paclitaxel, vinorelbine. Exfoliants Capable of causing inflammation and shedding of the skin; unlikely to cause tissue necrosis. Cisplatin, doxorubicin liposomal, docetaxel, oxaliplatin, topotecan. Irritants Capable of causing inflammation, irritation or pain, but rarely tissue necrosis. Carboplatin, etoposide, irinotecan. Inflammatory agents/ non-vesicants Capable of causing mild-to-moderate inflammation and flare in local tissue. Etoposide, fluorouracil, methotrexate. Neutrals Do not cause peripheral damage. Bleomycin, cyclophosphamide, gemcitabine, rituximab, trastuzumab, cisplatin, pemetrexed. (Hines 2011, Al-Benna et al 2013) Box 2 lists the signs and symptoms of an extravasation injury. Management strategies Management of these injuries depends on the drug used. Application of topical heat or cooling methods and extravasation antidotes are drug specific, and different interventions are indicated depending on the mechanism of action and the response to treatment. Initial management is to stop the infusion, keep the cannula in place, raise the alarm to obtain assistance and follow the local guidelines to manage the situation (Schulmeister 2010). Any clinical environment where cytotoxic agents are administered must have an extravasation kit available immediately should an incident occur. Local policies and guidelines are kept with the extravasation kit, in addition to essential information pertaining to the management of different chemotherapy extravasations, including the required medications and evidence-based algorithms (Figure 1). Complete time out activity 4 Other infusion-related toxicities There are other infusion-related side effects and toxicities associated with administering chemotherapy agents. The incidence of chemotherapy-induced nausea and vomiting and myelosuppression’s physiological effect are two of the most prominent risks and can cause significant complications. Myelosuppression and the risk of infection in particular can lead to fatal consequences if not identified and managed appropriately. Side effects such as mucositis can be severe and have detrimental effects on overall health and nutritional status,requiring medical intervention in extreme cases. Other symptoms such as bowel disturbance can be BOX 2 Signs and symptoms of an extravasation injury Altered sensation at the site of the cannula: – Tingling. – Burning. – Discomfort or pain. – Swelling. – Redness. Interruption to intravenous flow, resistance when administering a bolus injection and the absence of blood return may signal an extravasation injury. Late-stage symptoms may include blistering, necrosis and ulceration. (Schulmeister 2010) 56 february 17 from :: vol RCNi.com 30 no 25 by :: 2016 STANDARD Downloaded ${individualUser.displayName} on Aug 08, 2016. For personal use only. NoNURSING other uses without permission. Copyright © 2016 RCNi Ltd. All rights reserved. managed with prophylactic and therapeutic medication. Longer term problems that may arise and cause significant disruption to a patient’s general wellbeing and quality of life include hair loss, nail changes, peripheral neuropathy, taste changes, and cognitive and emotional problems. The more severe side effect of an increased risk of a thrombus is widely documented and can pose quite a significant complication (Livshits 2014). Patient education is essential to ensure an understanding of these physiological effects, FIGURE 1 Algorithm for the management of extravasation injuries during peripheral infusions Step 1 Stop and disconnect infusion. Leave the cannula in place. Step 2 Identify extravasated agent. Step 3 Leaving the cannula in place, try to gently aspirate as much extravasated solution as possible. Record volume removed in patient records. Avoid manual pressure over the extravasated area. Remove cannula. Step 4 Mark with a pen an outline of the extravasated area. Step 5 Notify physician. Start specific measures as soon as possible. Non vesicant Vesicant or irritant Localise and neutralise Agents: Anthracyclines Antibiotics (mitomycin/ dactinomycin) Alkylating agents Step 5A: Localise Apply dry cold compresses for 20 minutes 4 times daily for 1-2 days. Avoid alcohol compresses Step 5B: Neutralise Use specific antidotes Anthracyclines Topical DMSO Dexrazoxane Mitomycin C Topical DMSO Disperse and dilute Agents: Local dry cold compresses Vinca alkaloids Taxanes Platinum salts Step 5A: Disperse Apply dry warm compresses for 20 minutes 4 times daily for 1-2 days Step 5B: Dilute Administer agents increasing resorption Vinca alkaloids and taxanes Hyaluronidase Step 6 Elevate the limb. Administer analgesia if necessary. DMSO = Dimethyl sulfoxide (Pérez Fidalgo et al 2012, © European Society for Medical Oncology www.esmo.org/Guidelines) NURSING 17 other :: vol uses 30 no 25 :: permission. 2016 57 DownloadedSTANDARD from RCNi.com by ${individualUser.displayName} on Aug 08, 2016. For personal february use only. No without Copyright © 2016 RCNi Ltd. All rights reserved. CPD oncology and a discussion of management strategies and implications for treatment is a priority to prepare patients for therapy. It is beyond the scope of this article to provide detail on the delayed toxicities. Macmillan Cancer Support (2015) provides information on chemotherapy administration and targeted therapy, associated side effects and specific considerations. This resource can be used for patient education. Conclusion It is important that nurses have an understanding of the infusion-related risks associated with chemotherapy to recognise symptoms and ensure appropriate management strategies should complications occur. It should be noted that the information in this article provides an overview of a diverse subject, and further reading can provide additional knowledge NS Complete time out activity 5 USEFUL RESOURCES Bovelli D, Plataniotis G, Roila F; ESMO Guidelines Working Group (2010) Cardiotoxicity of chemotherapeutic agents and radiotherapy-related heart disease: ESMO Clinical Practice Guidelines. Annals of Oncology. 21, Suppl 5, 277-282. Bracci L, Schiavoni G, Sistigu A, Belardelli F (2014) Immune-based mechanisms of cytotoxic chemotherapy: implications for the design of novel and rationale-based combined treatments against cancer. Cell Death and Differentiation. 21, 1, 15-25. Lyman GH, Abella E, Pettengell R (2014) Risk factors for febrile neutropenia among patients with cancer receiving chemotherapy: a systematic review. Critical Reviews in Oncology/ Hemtaology. 90, 3, 190-199. Thompson N (2012) Optimizing treatment outcomes in patients at risk for chemotherapy-induced nausea and vomiting. Clinical Journal of Oncology Nursing. 16, 3, 309-313. 5 Now that you have completed the article, you might like to write a reflective account as part of your revalidation. Guidelines to help you are on page 62. References Al-Benna S, O’Boyle C, Holley J (2013) Extravasation injuries in adults. ISRN Dermatology. doi:10.1155/2013/856541. Gerber DE (2008) Targeted therapies: a new generation of cancer treatments. American Family Physician. 77, 3, 311-319. Castells MC, Matulonis UA (2015) Infusion Reactions to Systemic Chemotherapy. www.uptodate.com/ contents/infusion-reactions-tosystemic-chemotherapy (Last accessed: December 5 2015.) Gottlieb GR, Bordoni RE, Lawhead AR, Feinberg B (2010) Successful outpatient desensitization of cancer patients with hypersensitivity reactions to chemotherapy. Community Oncology. 10, 7, 452-457. Castells MC, Tennant NM, Sloane DE et al (2008) Hypersensitivity reactions to chemotherapy: outcomes and safety of rapid desensitization in 413 cases. Journal of Allergy and Clinical Immunology. 122, 3, 574-580. Chung CH (2008) Managing premedications and the risk for reactions to infusional monoclonal antibody therapy. The Oncologist. 13, 6, 725-732. Gatti L, Zunino F (2005) Overview of tumor cell chemoresistance mechanisms. Methods in Molecular Medicine. 111, 127-148. Hines A (2011) Network Guidance for the Prevention and Management of Extravasation Injuries. www. mccn.nhs.uk/userfiles/documents/ MCCN%20Extravasation_ final_Oct11.pdf (Last accessed: December 5 2015.) Kang SP, Saif MW (2007) Infusion-related and hypersensitivity reactions of monoclonal antibodies used to treat colorectal cancer – identification, prevention, and management. Journal of Supportive Oncology. 5, 9, 451-457. Lenz HJ (2007) Management and preparedness for infusion and hypersensitivity reactions. The Oncologist. 12, 5, 601-609. Livshits Z, Rao RB, Smith SW (2014) An approach to chemotherapy-associated toxicity. Emergency Medicine Clinics of North America. 32, 1, 167-203. Macmillan Cancer Support (2015) Chemotherapy. www.macmillan. org.uk/information-and-support/ treating/chemotherapy/ chemotherapy-explained (Last accessed: December 5 2015.) Malhotra V, Perry MC (2003) Models of anti-cancer therapy: classical chemotherapy. mechanisms, toxicities and the therapeutic window. Cancer Biology and Therapy. 2, 4, Suppl 1, S2-S4. Payne S, Miles D (2008) Mechanisms of Anticancer Drugs. http://cw.tandf. co.uk/scottbrownent/ sample-material/Chapter-4Mechanisms-of-anticancer-drugs. pdf (Last accessed: December 5 2015.) Pérez Fidalgo JA, García Fabregat L, Cervantes A et al (2012) Management of chemotherapy extravasation: ESMO-EONS Clinical Practice Guidelines. Annals of Oncology. 23, Suppl 7, 167-173. Repetto L (2003) Greater risks of chemotherapy toxicity in elderly patients with cancer. Journal of Supportive Oncology. 4, Suppl 2, 18-24. Schulmeister L (2010) Preventing and managing vesicant chemotherapy extravasations. Journal of Supportive Oncology. 8, 5, 212-215. Vogel WH (2010) Infusion reactions: diagnosis, assessment, and management. Clinical Journal of Oncology Nursing. 14, 2, E10-E21. Zetka ES (2012) The essentials of chemotherapy-induced infusion reactions. Clinical Journal of Oncology Nursing. 16, 5, 527-529. 58 february 17 from :: vol RCNi.com 30 no 25 by :: 2016 STANDARD Downloaded ${individualUser.displayName} on Aug 08, 2016. For personal use only. NoNURSING other uses without permission. Copyright © 2016 RCNi Ltd. All rights reserved. Downloaded from RCNi.com by ${individualUser.displayName} on Aug 08, 2016. For personal use only. No other uses without permission. Copyright © 2016 RCNi Ltd. All rights reserved. CPD assessment Chemotherapy: infusion risks TEST YOUR KNOWLEDGE BY COMPLETING SELF-ASSESSMENT QUESTIONNAIRE 831 1. Chemotherapy: a) Distinguishes between healthy and cancerous cells ❏ b) Causes cell death by inactivation of apoptosis ❏ c) Encompasses a range of cytotoxic agents to destroy cancer cells ❏ ❏ d) Targets tissue invasion 7. Which chemotherapy agent may result in laryngeal spasm following oxygen administration to treat an allergic reaction? a) Rituximab ❏ b) Oxaliplatin ❏ ❏ c) Taxane ❏ d) Etoposide 2. Which factor determines the success of chemotherapy? a) Presence of comorbidities b) Extent of the disease c) Overall patient health status d) All of the above 8. Which is not a risk factor associated with extravasation injury? a) Bolus medication administration ❏ ❏ b) Short infusion c) Medical problems associated with altered peripheral sensation ❏ d) Poor site selection ❏ 3. Which cytotoxic agent is most commonly associated with infusion-related reactions? a) Cetuximab b) Rituximab c) Paclitaxel d) Bevacizumab ❏ ❏ ❏ ❏ ❏ ❏ ❏ ❏ 4. To prevent tumour progression and growth in conjunction with chemotherapy agents, transduction inhibitors focus on: a) Epidermal growth factor receptors ❏ b) Gene expression modulators ❏ ❏ c) Hormones d) Apoptosis inducers ❏ 5. A symptom of an infusion-related reaction to chemotherapy is: a) Facial pallor ❏ b) Rapid respiratory rate ❏ c) Nausea ❏ d) Hypertension ❏ 6. When do most infusion-related reactions occur? a) Within 10 minutes of the initial administration ❏ b) Within 30 minutes of the initial administration ❏ c) Within 10 minutes of the initial or second administration ❏ d) Within 10 to 30 minutes of the initial or second administration ❏ 9. The class of chemotherapy agent with the potential to cause the most extravasation damage is: a) Vesicants ❏ b) Exfoliants ❏ ❏ c) Irritants ❏ d) Neutrals 10. Which statement is correct? a) Side effects such as mucositis may have detrimental effects on patients’ nutritional status ❏ b) Chemotherapy regimens always result in resistance to chemotherapy ❏ c) Monoclonal antibodies have a small risk of infusion-related reaction ❏ d) A n extravasation injury is always caused by misplacement of a peripheral cannula ❏ This self-assessment questionnaire was compiled by Noreen Begley The answers to this questionnaire will be published on March 2 How to use this assessment This self-assessment questionnaire (SAQ) will help you to test your knowledge. Each week you will find ten multiple-choice questions that are broadly linked to the CPD article. Note: there is only one correct answer for each question. You could test your subject knowledge by attempting the questions before reading the article, and then go back over them to see if you would answer any differently. might like to read the article to You update yourself before attempting the questions. When you have completed your self‑assessment, add it to your professional portfolio. You can record the amount of time it has taken. Space has been provided for comments. You might like to consider writing a reflective account, see page 62. Report back This activity has taken me _­­____ hours to complete. Other comments: Now that I have read this article and completed this assessment, I think my knowledge is: Excellent Good Satisfactory Unsatisfactory Poor As a result of this I intend to: ❏ ❏ ❏ ❏ ❏ The answers to SAQ 829 on acute pulmonary oedema, which appeared in the February 3 issue, are: 1. d 2. c 3. b 4. a 5. c 6. b 7. d 8. a 9. c 10. d 60 february 17 from :: volRCNi.com 30 no 25 by :: 2016 STANDARD Downloaded ${individualUser.displayName} on Aug 08, 2016. For personal use only. NoNURSING other uses without permission. Copyright © 2016 RCNi Ltd. All rights reserved.