SUL LIBRO: VITTORIO AGNOLETTO CARLO GNETTI AIDS: LO SCANDALO DEL VACCINO ITALIANO PREFAZIONE DI ROBERT GALLO CONSIDERAZIONI UTILI PER FARE CHIAREZZA Il libro contiene sia nella prefazione di Gallo sia nel corpo del testo falsità e distorsioni praticamente su tutto, incluso eventi, date, comunicazioni, fatti, ecc., ecc. Attacca senza esclusione di colpi, a destra e a sinistra, tutti i governi, i ministri, i politici, le istituzioni, gli scienziati, la ricerca italiana, le associazioni, la Commissione Nazionale AIDS, con considerazioni anche molto gravi sul Sudafrica e le sue capacità di regolamentazione e salvaguardia dei volontari. E’ un accanimento diffamatorio iniziato insieme da Gallo e Aiuti molti anni fa, continuato nel tempo, e che culmina ora con la pubblicazione di un libello diffamatorio con argomenti vecchi e notizie false sostenute sempre dagli stessi attori. La dott.ssa Ensoli, che ha lavorato con entrambi, li conosce molto bene e sa di che cosa sono capaci per ottenere visibilità. A questo riguardo si veda anche il libro su Gallo dal premio Pulitzer John Crewdson che fa una fedele ricostruzione del tentativo di Gallo di appropriarsi della paternità della scoperta del virus (All. 1 & 2). E’ palese l’intento del libro di diffamare non solo il vaccino, l’Istituto Superiore di Sanità (“ISS”) ed il suo Presidente, Prof. Garaci, ma anche le istituzioni pubbliche: Ministero della Salute ed i vari ministri che si sono succeduti negli anni, il Ministero degli Affari Esteri, il sottosegretario alla Presidenza del Consiglio Letta del governo Berlusconi, la Commissione Nazionale AIDS, gli scienziati e la ricerca pubblica italiana, e, in ultima analisi, il sistema Italia nel suo insieme che viene rappresentato come inaffidabile. Il libro ha una tale portata diffamatoria che viene naturale chiedersi per quali fini sia stato scritto, e se non ci siano dietro interessi economici/politici/internazionali che potrebbero beneficiare del fango che gli autori gettano sul sistema Italia. Un eventuale risposta point-­‐by point è semplicemente impossibile, poiché il libro contiene tante e tali falsità che ci vorrebbero mesi e 3 libri per rispondere. Il tono del libro è decisamente da giornale scandalistico e contiene numerosi spunti di natura “negazionista”. I FATTI Contrariamente a quello che dice Gallo, Barbara Ensoli è andata in USA nel gennaio del 1986, è una immunologa e lavora sul Tat sin dall’inizio della sua esperienza in USA: la sua prima pubblicazione sul Tat è su Nature nel 1987 e molte altre sono seguite da allora su questa proteina e su HIV sia negli Usa che in Italia (Allegato 4). I risultati della ricerca da Lei condotta sul Tat le hanno consentito di concepire e progettare un vaccino alternativo a quelli “canonici” basati sulla proteina virale Env, altamente mutabile, 1 utilizzando invece Tat, una proteina del virus altamente conservata e con funzioni chiave sull’infezione, molte delle quali scoperte proprio da lei (http://www.hiv1tat-­‐
vaccines.info/scientific_publications.htm) ( Allegato 4). Il Dr. Gringeri, contrariamente alle affermazioni di Gallo, ha iniziato molto più tardi a lavorare sul Tat e lo ha fatto utilizzando una proteina Tat modificata chimicamente per renderla biologicamente inattiva, e perciò denominata tossoide Tat, perché ritenuta da Gallo e collaboratori pericolosa nella sua forma naturale e biologicamente attiva (Gallo, Proc Natl Acad Sci USA 1999). Il tossoide Tat è pertanto ben diverso dalla proteina Tat biologicamente attiva volutamente usata dalla Dott.ssa Ensoli sulla scorta dei suoi studi di ricerca di base e dimostratasi innocua negli animali e poi nell’uomo. Il dott.Gringeri ha sperimentato il vaccino terapeutico basato sul tossoide Tat in uno studio “compassionevole” nell’uomo, ottenendo scarsi risultati che poi ha pubblicato sulla rivista Journal of Human Virology diretta da Gallo, (Gringeri et al., J. Hum. Virol 1998), praticamente un’autopubblicazione. Da notare che il Dr. Gringeri ha condotto lo studio senza aver ottenuto l’approvazione da parte delle autorità regolatorie. In relazione alle insinuazioni del libro relative al Programma Nazionale AIDS, all’epoca del rientro della dott.ssa Ensoli in Italia esso era coordinato dalla Prof.ssa Verani dell’ISS, mentre la dott.ssa Ensoli è subentrata solo dopo vari anni come Coordinatore. Il Programma è sempre stato gestito dall’ISS secondo i criteri di peer-­‐review con revisori esterni che hanno valutato i progetti in forma anonima e con una commissione che in trasparenza ha classificato i progetti secondo i risultati del processo di revisione esterno, premiando i migliori. Di questa commissione il Prof. Fernando Aiuti ha fatto parte per molti anni. CV breve della Dr.ssa Barbara Ensoli Direttore del Centro Nazionale AIDS, Istituto Superiore di Sanità, Roma, Italia. Barbara Ensoli, MD, Ph.D., si è laureata in Medicina e Chirurgia e specializzata in Immunologia Clinica e Allergologia presso l'Università di Roma "La Sapienza", Italia. Ha poi trascorso circa 11 anni presso i National Institutes of Health (Bethesda, Maryland, USA), lavorando al National Cancer Institute. In questi anni ha studiato il ruolo della proteina Tat di HIV-­‐1 nella patogenesi dell'HIV e nei tumori associati all’AIDS. I suoi attuali interessi di ricerca sono diretti alla patogenesi dell’HIV e allo sviluppo di vaccini preventivi e terapeutici contro HIV / AIDS, attualmente in fase clinica avanzata. Ha coordinato numerosi programmi di ricerca nazionali, in Europa e nei paesi in via di sviluppo. Tra questi, l’ "AIDS Vaccine Integrated Project" (AVIP), finanziato dall'Unione Europea, e il "Programma di sostegno al Ministero della sanità del Sudafrica per l'attuazione di un programma nazionale di risposta globale all'HIV e AIDS", finanziato dal Ministero degli Affari Esteri italiano, che è attualmente in corso. Barbara Ensoli è membro della Vaccine Advisory Committee dell’OMS-­‐Unaids. E’ il Vice-­‐Presidente della Commissione Nazionale AIDS del Ministero della Salute, fa parte dell’editorial board di numerose riviste internazionali ed ha ricevuto molti riconoscimenti scientifici nazionali e internazionali. E’ stata nominata Ufficiale dell'Ordine al Merito della Repubblica Italiana nel 2001 dal Presidente della Repubblica Italiana, On. A. Ciampi. Le sue attività scientifiche annoverano a più di 300 pubblicazioni in riviste internazionali peer-­‐
reviewed di cui più di 120 su Tat ed HIV (Allegato 4). 2 LO SVILUPPO DEL VACCINO dell’ISS IN SINTESI (http://www.iss.it/aids/;http://www.hiv1tat-­‐vaccines.info/ ) Gli studi vaccinali su Tat In Italia sono stati iniziati da Barbara Ensoli all’Istituto Superiore di Sanità utilizzando al meglio l’eccellente piattaforma preclinica presente in Istituto e sulla base del suo bagaglio di conoscenze e scoperte frutto della propria ricerca, effettuata negli anni precedenti negli USA, e di cui Gallo ha grandemente beneficiato (Allegato 4). La ricerca in Italia è iniziata con gli studi preclinici nelle scimmie, il modello animale di riferimento per lo sviluppo di vaccini contro l’HIV. I risultati degli studi nelle scimmie sono stati pubblicati su riviste internazionali peer-­‐reviewed (Cafaro et al., Nat Med 1999; Cafaro et al., J Med Primatol 2000; Cafaro et al., Vaccine 2001; Maggiorella et al., Vaccine 2004; Mooji et al., J Virol 2004; Cara et al., Virology 2004; Demberg et al., J Virol 2007; Demberg et al, Vaccine 2008; Ridolfi et al, Virus Genes 2008; Fanales-­‐Belasio et al., J Immunol 2009; Florese et al., J Immunol 2009; Borsetti et al., Viral Immunol 2009; Cafaro et al., J Virol 2010; Ferrantelli et al., Vaccine 2011; Monini et al., PLoS ONE 2012). Sulla base degli ottimi risultati ottenuti nelle scimmie sono state allestite tutte le piattaforme necessarie alla conduzione di studi clinici nell’uomo, inclusa la produzione in condizioni di GMP del vaccino Tat (Fig. 1). Gli studi di fase I sono iniziati dopo l’approvazione dei protocolli da parte dei Comitati Etici e della commissione del Comma C (DM 21/12/2007; D.Lgs. 211/2003). I due studi sono stati registrati sull’osservatorio internazionale degli studi clinici (Clinicaltrials.gov identifier: ISS P-­‐001, NCT00529698; ISS T-­‐001, NCT01024595). Sono state condotte due sperimentazioni multicentriche (uno studio preventivo, “ISS P-­‐001”, su 20 soggetti, uno terapeutico, “ISS T-­‐001”, su 27 soggetti) che hanno confermato che il vaccino Tat è sicuro ed immunogenico (Clinicaltrials.gov identifier: ISS P-­‐001, NCT00529698; ISS T-­‐001, NCT01024595). I risultati sono stati pubblicati su riviste internazionali peer-­‐reviewed (Ensoli, AIDS 2006, Ensoli, AIDS 2008, Vaccine 2009; Longo, Vaccine 2009; Bellino RRCT 2009; Luzi, AIDS Care 2010). I rapporti finali ufficiali dei due studi sono stati inviati, come richiesto dalla legge, al Ministero della Salute e ai Comitati Etici dei centri clinici partecipanti agli studi. Il programma di sviluppo clinico del candidato vaccinale basato sulla proteina Tat è proseguito, previa approvazione da parte del Comitato Etico coordinatore e di quelli degli 11 centri clinici italiani partecipanti, con una sperimentazione clinica terapeutica di fase II su 168 pazienti in terapia antiretrovirale efficace (ISS T-­‐002, EudraCT number: 2007-­‐007200-­‐16; Clinicaltrials.gov identifier: NCT00751595). Lo studio, completato recentemente, non solo ha confermato la sicurezza e l’immunogenicità del vaccino, ma ha anche dimostrato efficacia per la ricostituzione del sistema immune dei pazienti. I risultati preliminari sono stati pubblicati su PLoS ONE (Ensoli, PLoS ONE 2010), una rivista scientifica peer-­‐review internazionale, fondata, con altri scienziati, dal premio Nobel Harold Varmus che è stato anche per molti anni il Direttore degli NIH. La rivista è altamente apprezzata 3 dal mondo scientifico accademico internazionale e dall’attivismo, in quanto accessibile a tutti gratuitamente e risponde alla filosofia che l’accesso al sapere e alle conoscenze deve essere libero, universale e per l’appunto, gratuito. I dati di efficacia a lungo termine dello studio di fase II, fino a 144 settimane dalla prima vaccinazione, sono oggetto di due pubblicazioni in corso di preparazione, incentrate, rispettivamente, sugli aspetti di efficacia virologica e di immunoricostituzione indotti dal vaccino. Il rapporto finale ufficiale dello studio sarà inviato, in accordo alle specifiche di Legge, all’AIFA e ai Comitati Etici dei centri clinici partecipanti agli studi. L’insieme delle ricerche effettuate, dei risultati dei protocolli vaccinali e della ricerca di base ha portato alla recentissima pubblicazione del meccanismo di azione del vaccino Tat (Monini, PLoS ONE, 2012), che spiega le ragioni per le quali i vaccini sperimentati precedentemente e basati su Env o altri antigeni strutturali hanno dato risultati fallimentari o marginali (Fuchs et al, J Acquir Immune Defic Syndr 2010). Questi dati confermano la necessità di impostare nuove strategie vaccinali. Gli studi appena pubblicati dal laboratorio della Dr.ssa Ensoli, in collaborazione con numerosi centri di ricerca italiani e con Novartis, indicano che un vaccino terapeutico deve contenere solo il Tat, mentre un vaccino preventivo richiede che Tat sia combinato con una proteina Env nella forma presente sul virus. Uno studio nell’uomo di fase I con un vaccino combinato di Tat ed Env (sicurezza ed immunogenicità sono gli indicatori primari) è al momento in corso in 3 centri clinici in Italia (ISS P-­‐002, EudraCT number: 2008-­‐007224-­‐26; Clinicaltrials.gov identifier: NCT01441193) Strettamente connesso al programma di studi clinici in Italia, perché basato sui risultati ottenuti in Italia negli studi di fase I e nello studio di fase II, è lo studio terapeutico di fase II su soggetti in terapia antiretrovirale (ISS T-­‐003, Clinicaltrials.gov Identifier:NCT01513135), avviato di recente in Sudafrica nell’ambito di un programma di cooperazione tra Italia e Sudafrica finanziato dal MAE. A fine arruolamento i soggetti vaccinati saranno 200. Tutti gli studi clinici si sono avvalsi della consulenza di esperti internazionali, membri dei rispettivi Scientific Advisory Board, che hanno seguito gli studi durante il loro svolgimento e ne hanno valutato i risultati (Fig. 1). Il vaccino Tat ad oggi è stato somministrato a 309 volontari. La sua sicurezza ed immunogenicità è stata confermata dal Data Safety Monitoring Board (DSMB), un comitato indipendente e internazionale che valuta e analizza per ogni trial tutti i risultati relativi alla sicurezza della vaccinazione (Fig. 1). Tutti i report sono stati regolarmente inviati ai comitati etici e all’AIFA come richiesto da legge. Inoltre, secondo gli standard (in realtà non troppo applicati) internazionali previsti per ogni studio, è stato istituito un Community Advisory Board (“CAB”) formato dalle principali associazioni di pazienti di lotta all’AIDS e/o delle comunità colpite dall’infezione al fine di condividere e confrontarsi sulle procedure che riguardavano direttamente il benessere dei volontari nonché condividere i risultati in itinere (Fig. 1). Ogni studio clinico è stato seguito da una CRO (Clinical Research Organization come per esempio Parexel) per il monitoraggio, la conduzione ed il controllo dei requisiti di qualità, coerentemente 4 con quanto richiesto dalle Good Clinical Practice, di ogni studio clinico. La presenza della CRO è un requisito di legge per la conduzione di studi clinici (Fig. 1). Gli studi sono stati tutti condotti nel rispetto delle leggi concernenti la sperimentazione clinica in Europa. In Sudafrica lo studio clinico è stato approvato dalla Medicines Control Council, una delle agenzie regolatorie tra le più severe al mondo e di alta qualità. In sintesi, lo stato dell’arte della sperimentazione clinica del vaccino Tat è illustrata in Fig. 2 & 3. Come mostrato in Fig. 3, lo stato di sviluppo del vaccino è molto avanzato ed, in particolare per il vaccino terapeutico, occorre solamente la fase III di sperimentazione clinica per accedere all’iter registrativo e quindi alla sottomissione del dossier (Common Technical Document, CTD) alle autorità regolatorie per richiederne l’autorizzazione all’immissione in commercio. I dati delle sperimentazioni sono già stati discussi con l’AIFA. IL BUDGET DEL PROGETTO VACCINO AD OGGI I dati riportati di seguito includono i costi diretti dei vari progetti, incluso personale dedicato; escludono i costi del personale di ruolo dell’ISS che ha collaborato al progetto. Ricerca di Base e Preclinica Il budget della ricerca preclinica dal 1995 sino alla prima approvazione per l’uso nell’uomo ammonta ad un totale di circa € 20 milioni, che, sottratti di IVA e spese generali, si riducono a circa € 14 milioni. La tabella che segue riassume le fonti di finanziamento. Fonti dei finanziamenti per la Ricerca di Base e Preclinica Fonti nazionali • Grants per progetti peer-­‐
• Programma nazionale AIDS (Ministero della Salute) reviewed con revisori • AIRC (Fondazione privata) esterni • Ricerca finalizzzata (Ministero della Salute) • FIRB (Ministero della Ricerca) • Programma Italia-­‐USA (Ministero della Salute) Fonti internazionali • Progetti Europei • AVIP (coordinato da ISS) • VIAV (coordinato da ISS) • Muvapred (coordinato da Novartis) • Europrise (coordinato da CE) Progetti in collaborazione con • ISS-­‐Chiron/Novartis (Ministero della Salute) l’Industria 5 Sperimentazione clinica Il costo medio industriale dello sviluppo di un vaccino, un qualsiasi vaccino per uso nell’uomo, è stato stimato a circa $500 milioni1, circa €400 milioni al cambio di oggi. Per il programma vaccino Tat, i fondi ottenuti dal Ministero della Salute e da ISS ed utilizzati per la sperimentazione clinica in Italia ammontano a €15,75 milioni, che, sottratti di IVA e spese generali, si riducono a circa €11,25 milioni, una piccola frazione rispetto a quanto spende un’industria privata per raggiungere lo stato avanzato di sviluppo raggiunto con il vaccino Tat (Fig. 3). Se si considera che con circa 30 milioni di euro sarà possibile completare lo sviluppo clinico del vaccino terapeutico sino alla registrazione, i fondi impiegati sinora ammontano a circa un decimo di quelli medi industriali. Con i circa €11,25 milioni sono stati effettuati i seguenti studi, completati e/o in corso, che comprendono la messa a punto di tutte le piattaforme richieste, inclusa la produzione GMP, il testing del prodotto, l’inflaconamento, i trasporti GMP etc. etc. • Studio di fase I preventiva (20 soggetti) • Studio di fase I preventiva con follow up a 5 anni come studio osservazionale • Studio di fase I terapeutica (27 soggetti) • Studio di fase I terapeutica con follow up a 5 anni come studio osservazionale • Studio di fase II terapeutica (168 soggetti) • Studio di fase II terapeutica con follow-­‐up a 5 anni, come studio osservazionale • Studio osservazionale di controllo per la fase II terapeutica (88 soggetti, dei 144 arruolati e seguiti nello studio) • Studio osservazionale su soggetti infettati asintomatici per studiare la progressione della malattia (73 soggetti) I fondi per gli studi in Sudafrica sono stati ottenuti dal MAE, nell’ambito di un programma di cooperazione con il governo sudafricano di cui lo studio è una delle 3 componenti: 1. La componente 1 ha l’obiettivo di rafforzare il sistema sanitario per la lotta contro l’AIDS nei siti prescelti dal National Department of Health (“NDOH”, che è l’equivalente del Ministero della Salute in Italia); sono ivi inclusi i siti per la sperimentazione clinica che impone standard di qualità altissimi e infrastrutture cliniche adeguate. Gli studi clinici previsti includono uno studio osservazionale, denominato ISS OBS T-­‐004, volto alla caratterizazione dell’infezione da HIV e delle principali co-­‐infezioni in 700 volontari con o senza trattamento antiretrovirale per valutare l’impatto della terapia e aderenza dei pazienti alla stessa. Il programma comprende anche lo screening di HPV nelle donne. 2. La componente 2 ha l’obiettivo di trasferire al Biovac Institute, una struttura pubblico-­‐
privata partecipata dal NDOH, la tecnologia di produzione di vaccini ricombinanti in Sudafrica utilizzando Tat come primo vaccino per la validazione da parte delle agenzie regolatorie sudafricane del sito produttivo. 3. La componente 3 è la sperimentazione terapeutica di fase II nei siti oggetto delle attività della componente 1 a prova dell’avvenuto rafforzamento con standard di eccellenza dei siti clinici. 1http://www.iavireport.org/Back-­‐Issues/Pages/IAVI-­‐Report-­‐14%282%29-­‐InvestinginSurprise.aspx) 6 Il budget complessivo per il programma di cooperazione in Sudafrica è di €22,34 milioni; di questi, €2.1 milioni sono destinati alle attività di monitoraggio e valutazione di impatto del programma stesso da parte del MAE e NDOH, mentre €20,24 sono destinati alle attività delle 3 componenti, che, sottratte le spese generali, si riducono a circa €18,4 milioni. La ripartizione del budget di tutto il programma di cooperazione in Sudafrica è la seguente: • € 6,9 milioni per la componente 1 • € 4,0 milioni per la componente 2 • € 7,5 milioni per la componente 3, ossia lo studio clinico e le attivita’ di supporto necessarie alla sua preparazione ed esecuzione Il budget per gli studi di ricerca di base e preclinica di Tat ed Env provengono da programmi di ricerca italiani e progetti europei coordinati dalla Dr.ssa Ensoli quali AVIP, VIAV e per lo studio clinico del vaccino preventivo Tat/Env, in parte dalla comunità europea ed in parte dal Ministero della Salute (sempre parte degli stessi fondi di cui sopra). Il budget della sperimentazione clinica in Italia e Sudafrica e le fonti di finanziamento sono rappresentate nella tabella che segue. Budget della sperimentazione clinica e fonti di finanziamento Studio Clinico Fonte di Finanziamento (al netto di IVA e spese generali) ITALIA • ISS: € 1 M • Fase I, Tat preventivo & terapeutico • Min. della Salute € 11,25 M • Fase II, Tat terapeutico in HAART Subtotale € 12,25 M • Fase I Tat/Env, Italia SUDAFRICA* • Min. degli Affari Esteri: € 7,5 M • Fase II, terapeutico Totale € 19,75 M *: costi della componente 3 (studio clinico) Tutti i fondi impiegati nelle sperimentazioni su descritte sono stati tutti rigorosamente e puntualmente rendicontati all’istituzione di provenienza e sottoposti all’approvazione da parte della Corte dei Conti. 7 CONSIDERAZIONI CONCLUSIVE I risultati ottenuti sinora indicano che la strategia dell’ISS è corretta ed accurata, e che il completamento delle sperimentazioni e la successiva approvazione per la commercializzazione porterà il vaccino alla gente, di tutto il mondo. Il programma è stato portato avanti con costi che sono un decimo (Rif dati IAVI) rispetto a quelli che impiega l’industria per raggiungere gli stessi risultati. Ciò grazie alle conoscenze, ai test di laboratorio e ai reagenti specifici sviluppati dalla dott.ssa Ensoli, alle grandi capacità scientifiche dell’ISS, all’accuratissimo coordinamento del programma e ai molti sacrifici di tutti gli attori, incluse le associazioni di pazienti e/o comunità colpite e attivamente coinvolte nel programma. I risultati ottenuti sono stati sottoposti al vaglio della comunità scientifica (peer-­‐review) che ne ha confermato la serietà, come dimostrato dalla loro pubblicazione, a partenza dall’Italia, in oltre 50 articoli su riviste internazionali (http://www.hiv1tat-­‐vaccines.info/scientific_publications.htm). La correttezza della sperimentazione è stata accertata dagli organi competenti (Comitati etici, Comma C, DSMB, AB, AIFA, MCC) che ne hanno attestano l’assoluta conformità GMP e GLP (Good Manufacturing Practice e Good Laboratory Practice) secondo la regolamentazione in Italia, EU e Sudafrica. L’accanimento contro le istituzioni italiane (ISS, MIN SAL, MAE) è senza senso, immotivato, dannoso alla ricerca pubblica, ai pazienti e alle comunità particolarmente colpite dall’infezione da HIV. Un attacco così orchestrato è anche contro un potenziale intervento di salute pubblica, di risparmi di risorse e benessere, che un prodotto come quello prospettato ci attendiamo porterà. Il “progetto vaccino Tat terapeutico”, quello più avanzato, se arriverà con successo alla registrazione, comporta per l’Italia almeno: • Una riduzione dei costi per il SSN perché migliorerà la qualità del sistema immune dei pazienti e diminuirà la frequenza delle sindromi associate (causa di ospedalizzazione e morte) • Un ritorno economico e prestigio nel mondo per la ricerca italiana Il “progetto vaccino Tat/Env preventivo”, se arriverà con successo alla registrazione, avrà un forte impatto positivo sui sistemi sanitari nazionali di tutto il mondo, in particolare quelli dei paesi emergenti, con profonde implicazioni sulle economie nazionali e sullo stato sociale dei vari paesi convolti. Forse sono questi i risultati che si vogliono impedire e distruggere. A parte i motivi personali di Gallo, Aiuti e Agnoletto, ci chiediamo chi è veramente dietro a tutto questo? Quali lobby stanno operando? Dove vogliono arrivare? Allegati: 1. Articolo re indagine su Gallo 2. Science Fictions: A Scientific Mystery, a Massive Cover-­‐Up, and the Dark Legacy of Robert Gallo 3. Articolo re vaccino Gallo 4. Lista pubblicazioni su Tat ed HIV della Dr. Ensoli 8 Fig. 1
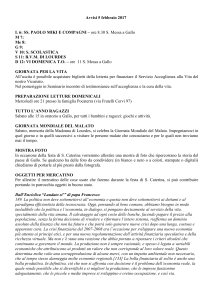
Tat vaccine Phase II clinical trial network
CRO
ISS
Sponsor
International
Advisory Board
(IAB)
Clinical Platform
Laboratory Platform
Psychological
Platform
Clinical Sites
Core Lab Immunology
and Virology
Psychologists at
clinical sites
Project Manager
CRA
Safety Monitoring
Data Safety
Monitoring Board
(DSMB)
Communication
AIDS Help
Line
(TVA)
Community
Advisory Board
(CAB)
Fig. 2
The Tat vaccine is safe and immunogenic in both seronegative and HIV-infected
individuals on or off HAART
Phase I preventive trial, randomized, double blind, placebo
controlled (ISS P-001), Italy
20
Phase I therapeutic trial, randomized, double blind, placebo
controlled (ISS T-001), Italy
27
Phase II therapeutic trial, randomized, open label
168
(ISS T-002), Italy
Phase II therapeutic trial, randomized, double blind placebo
controlled (ISS T-003) (ongoing, 200), South Africa
84
Phase I preventive trial, randomized, open label
10
(ISS P-002) (ongoing,50), Italy
Total vaccinated individuals
Ensoli B. et al. AIDS 2006, Ensoli B. et al. AIDS 2008, Ensoli B. et al. Vaccine 2009,
Longo O. et al. Vaccine 2009, Bellino S. et al. Reviews on Recent Clinical Trials 2009,
Luzi A.M. et al. AIDS Care 2011, Ensoli B et al. PLoS ONE 2010.
309
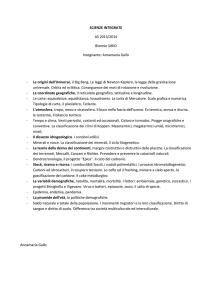
Fig. 3
HIV Tat Vaccines Development Plan
2012
1995
Candidate
development
GMP
Approval
Pre-clinical Production
for
studies
& testing Human use
Phase I
2013
Phase II
2016
Phase
Phase
III III
Approval for
Registration &
Marketing
PREVENTATIVE TAT+ENV VACCINE :
completed; phase I trial ongoing in IT
Discovery
THERAPEUTIC TAT VACCINE:
completed in Italy; phase II trial ongoing in S.Africa
PLANNED
ALLEGATO 1
ALLEGATO 2
Reviews
edited by Stephanie Deming
Science Fictions,
Journalistic
Obsessions
SCIENCE FICTIONS: A SCIENTIFIC MYSTERY, A
MASSIVE COVER-UP, AND THE DARK LEGACY
OF ROBERT GALLO. JOHN CREWDSON. BOSTON:
LITTLE, BROWN AND COMPANY; 2002. 670
PAGES. HARDCOVER $27.95. ISBN 0-31613476-7.
In early 1981, young men were being admitted to hospitals in California with a bizarre
syndrome that would later be called acquired
immunodeficiency syndrome, or AIDS. To
virologists, it was obvious or intuitive that
an unknown virus was causing the illness.
One of them, Robert Gallo, at the National
Institutes of Health (NIH), had discovered
the human T-cell lymphoma virus (HTLV)
in a patient with mycosis fungoides, a T-cell
skin cancer, several years previously. He
wanted his next discovery to be the virus
that caused AIDS, and he was convinced
from the start that it was another HTLV. At
almost precisely the same time in the early
1980s, virologists at the Institut Pasteur in
Paris under the direction of Luc Montagnier
were also searching for viruses in the blood
of patients with AIDS. Both Gallo and
Montagnier found a virus. Claims of precedence were important, not just for reasons of
vanity (and the potential for a Nobel Prize)
but also for patent rights on the HIV test.
What followed is the subject of this book:
a decade of scientific dispute, alleged (and
some proven) scientific misconduct by
Gallo and colleagues, investigations by the
Office of Research Integrity in the United
States, a congressional investigation, and
even meetings between the presidents of
France and the United States.
In early 1983, Montagnier had found the
virus now called HIV in a patient. He was
preparing his paper for submission to Nature
when he received a call from Gallo. Gallo
and his colleagues at NIH had isolated an
HTLV from a patient with AIDS and were
preparing to send the report to Science.
Montagnier was convinced that the virus he
had discovered was not an HTLV, and his
paper made this clear. However, he agreed to
switch journals and sent Gallo a copy of his
paper to send on to Science. But Montagnier
had neglected to write an abstract. In the
rush to get the papers to Science, Gallo
wrote the abstract for Montagnier; however,
the abstract written by Gallo indicated that
the French scientists had also discovered an
HTLV, thus in a sense confirming Gallo’s
discovery. Montagnier never saw the
abstract until the paper had been published.
In the postpublication fanfare—the popular press proclaimed the discovery of the
cause of AIDS—Gallo got the credit. The
Montagnier paper was largely ignored.
Thus began a long, confusing, and, in the
end, tragic episode in the scientific history of
AIDS—tragic, because the dispute between
Gallo and Montagnier delayed for almost a
decade scientific and clinical acceptance of
the idea that AIDS was caused by HIV, the
virus that Montagnier had found in January
1983.
Gallo finally admitted that he had the
wrong virus and Montagnier had the right
one. But Gallo then claimed that he had
also discovered HIV and that he had done
this (but not published his finding) before
Montagnier’s discovery. This also was
untrue. As was common among virologists, the two investigators had exchanged
samples and tissue cultures. Not all HIVs are
alike—in fact, they are remarkably different
in their genomic sequences. When genetic
analyses were finally done, it was shown
that the French and US viruses were not
only similar but identical. They must have
come from the same patient, and that was
the patient first investigated by Montagnier
years previously. Purposely or through negligence, Gallo had “discovered” Montagnier’s
virus.
This is a great story of scientists pursuing
not so much truth as fame. There are wonderful accounts of how high-flying scientists
like Gallo (in the period 1983-1994 he
published, according to my PubMed search,
over 70 papers per year—more than one per
week!) negotiated with editors and how editors were influenced. For example, shortly
after the Science papers were published,
another virologist, David Purtilo, had
tried to publish data showing that when he
examined blood samples from patients with
AIDS he failed to find any evidence of the
Gallo virus. Science turned Purtilo’s paper
Science Editor • November - December 2002 • Vol 25 • No 6 • 199
Reviews
continued
down—and so did George Lundberg at the
Journal of the American Medical Association,
who ignored the author’s cover-letter statement that “the undocumented implication
that this virus (HTLV) causes AIDS has
grave consequences to all of the individuals
at risk for AIDS.” The paper was eventually published in AIDS Research, a small
and then-obscure journal edited by Joseph
Sonnabend, a Greenwich Village physician
who had a large practice devoted to AIDS
patients. The paper was ignored.
Purtilo was correct, but for the next
8 years, the world was convinced that
the cause of AIDS was an HTLV. Then,
under increasing pressure from several sources—including the NIH Office of
Scientific Integrity, which had begun an
investigation into Gallo’s AIDS research,
and a congressional investigation led by
John Dingell—Gallo admitted that “his”
virus was indeed the “French” virus that
had somehow “accidentally” contaminated
cultures in his laboratory.
Not only did those events confuse scientists, clinicians, and patients, but they
delayed implementation of an effective
and sensitive blood test for HIV. Abbott
Laboratories in the United States and the
Institut Pasteur in France had each developed an AIDS test. Abbott used as its starting point a virus it had obtained from Gallo.
The French, of course, used the correct virus
from Montagnier. Abbott’s test had low
sensitivity, falsely reassuring patients that
they did not have AIDS and letting thousands of HIV-infected blood donors in the
United States continue to donate.
Not all readers will enjoy this book. It
is not a biography: after almost 600 pages
of dense text, we know little about Robert
Gallo other than his penchant for first-class
travel and his affair with his collaborator,
Flossie Wong-Staal. But that is about all.
We really don’t get much of an explanation
of why Gallo was so intent on getting credit
200 • Science Editor • November - December 2002 • Vol 25 • No 6
for the discovery of the AIDS virus—why
fame seemed so much more important
to him than truth. What author John
Crewdson does provide reads a little like
a police dossier or a presidential impeachment file. The writing style is almost staccato in its presentation of data, all of which
are meticulously cataloged. The footnotes
run to 100 pages in very small type. And
the text is further backed up by a Web
site (www.sciencefictions.net) that includes
what must be thousands of references (each
numbered to correspond to the cited text
reference) and a huge list of documents
in PDF, most of which were obtained by
Crewdson under freedom-of-information
legislation. One can, for example, read copies of memos from Wong-Staal to Gallo,
along with reports of the Office of Research
Integrity.
But I liked the book. In fact, flying to
San Diego to attend the recent meeting of
the Council of Science Editors, I couldn’t
put it down (or found it much preferable
to the in-flight film). Crewdson, a Pulitzer
Prize–winning journalist, first broke the
story that the Gallo virus was identical with
or very similar to the French virus (and
reproduced the DNA nucleotide sequences
that had been added to a database only a
few weeks previously) in a 55,000-word
article in the Chicago Tribune in November
1989. Writing this exhaustive book must
have occupied most of the next 12 years
of his life. The author’s motivation? One
might conclude that he was simply obsessed
with Gallo. But perhaps he was trying to be
as meticulous and accurate with his reporting of science as Gallo was sloppy or deliberately misleading with his doing of it.
John Hoey
JOHN HOEY is Editor of CMAJ: Canadian
Medical Association Journal.
ALLEGATO 3
Allegato 4
Pubblicazioni della Dr. Barbara Ensoli su Tat ed HIV
1. Arya S.K., Beaver B., Jagodzinski L., Ensoli B., Kanki P.J., Albert J., Fenyol E.M., Biberfeld
G., Zagury J.F., Laure F., Essex M., Norrby E., Wong-Staal F., and Gallo R.C. New human and
simian HIV related retroviruses posses functional transactivator (tat) gene. Nature 328: 548-550,
1987.
2. Fisher A., Ensoli B., Ivanoff L., Chamberlain M., Petteway S., Ratner L., Gallo R.C., and
Wong-Staal F. The sor gene of HIV-1 is required for efficient virus transmission in vitro.
Science 237: 888-893, 1987.
3. Fisher A.G., Ensoli B., Looney D., Rose A., Gallo R.C., Saag M.S., Shaw G.M., Hahn B.H.,
and Wong-Staal F. Biologically diverse molecular variants within a single HIV-1 isolate. Nature
334: 444-447, 1988.
4. Nakamura S., Salahuddin S.Z., Biberfeld P., Ensoli B., Markham P.D., Wong-Staal F., and
Gallo R.C. Kaposi's sarcoma cells: Long-term culture with growth factor from retrovirusinfected CD4+ T cells. Science 242: 426-430, 1988.
5. Ensoli B., Nakamura S., Salahuddin S.Z., Biberfeld P., Larsson L., Beaver B., Wong-Staal F.,
and Gallo R.C. AIDS-Kaposi's sarcoma-derived cells express cytokines with autocrine and
paracrine growth effects. Science 243: 223-226, 1989.
6. Lusso P., Ensoli B., Markham P.D., Ablashi D.V., Salahuddin S.Z., Tschachler E., Wong-Staal
F., and Gallo R.C. Productive dual infection of human CD4+ T lymphocytes by HIV-1 and
HHV-6. Nature 337:370-373, 1989.
7. Ensoli B., Lusso P., Schachter F., Josephs S.F., Rappaport J., Negro F., Gallo R.C., and WongStaal F. Human herpes virus-6 increases HIV-1 expression in co-infected T cells via nuclear
factors binding to the HIV-1 enhancer. EMBO J. 8:3019-3027, 1989.
8. Ensoli B., Salahuddin S.Z., and Gallo R.C. AIDS-associated Kaposi's sarcoma: A molecular
model for its pathogenesis. Cancer Cells 1:93-96, 1989.
9. Lusso P., Di Marzo Veronese F., Ensoli B., Franchini G., Jemma C., DeRocco S.E.,
Kalyanaraman V.S., and Gallo R.C. Expanded HIV-1 cellular tropism by phenotypic mixing
with murine endogenous retroviruses. Science 247:848-852, 1990.
10. Ensoli B., Barillari G., Salahuddin S.Z., Gallo R.C., and Wong-Staal F. Tat protein of HIV-1
stimulates growth of cells derived from Kaposi's sarcoma lesions of AIDS patients. Nature
344:84-86, 1990
11. Ensoli B. and Gallo R.C. Kaposi's sarcoma and AIDS. Nature 346:801-802, 1990.
12. Lusso P., Di Marzo Veronese F., Ensoli B., Franchini G., Jemma C., DeRocco S.E.,
Kalyanaraman V.S., and Gallo R.C. Pseudotypes in HIV-1 infected mice. Science 250: 11521154, 1990.
1
13. Barillari G., Buonaguro L., Fiorelli V., Hoffman J., Michaels F., Gallo R.C., and Ensoli B.
Effects of cytokines from activated immune cells on vascular cell growth and HIV-1 gene
expression. Implications for AIDS-Kaposi's sarcoma pathogenesis. J. Immunol. 149: 3727-3734,
1992.
14. Buonaguro L., Barillari G., Chang H.K., Bohan C.A., Kao V., Morgan R., Gallo R.C., and
Ensoli B. Effects of the human immunodeficiency virus type 1 Tat protein on the expression of
inflammatory cytokines. J. Virol. 66: 7159-7167, 1992.
15. Ensoli B. and Gallo R.C. Growth factors in AIDS-associated Kaposi's sarcoma: Cytokines and
HIV-1 Tat protein. In DeVita V.T., Hellman S., and Rosenberg S.A. (Eds.): AIDS Updates, Vol.
5, n. 2, J.B. Lippincott Company, Philadelphia, 1992, pp. 1-7.
16. Bohan C.A., Kashanchi F., Ensoli B., Buonaguro L., Boris-Lawrie K.A. and Brady J. Analysis
of Tat transactivation of human immunodeficiency virus transcription in vitro. Gene Expr. 2:
391-407, 1992.
17. Ensoli B., Buonaguro L., Barillari G., Fiorelli V., Gendelman R., Morgan R.A., Wingfield P.,
and Gallo R.C. Release, uptake, and effects of extracellular Human Immunodeficiency Virus
type 1 Tat protein on cell growth and viral transactivation. J. Virol. 67: 277-287, 1993.
18. Barillari G., Gendelman R., Gallo R.C., and Ensoli B. The Tat protein of human
immunodeficiency virus type 1, a growth factor for AIDS Kaposi sarcoma and cytokineactivated vascular cells, induces adhesion of the same cell types by using integrin receptors
recognizing the RGD amino acid sequence. Proc. Natl. Acad. Sci. USA 90: 7941-7945, 1993.
19. Ensoli B. and Gallo R.C. Growth factors in AIDS-associated Kaposi's sarcoma: Cytokines and
HIV-1 Tat protein. In DeVita V.T. Jr., Hellman, S., and Rosenberg, S.A. (Eds.): AIDS Updates,
Vol. 7, n. 1, J.B. Lippincott Company, Philadelphia, 1994, pp. 1-12.
20. Buonaguro L., Buonaguro F.M., Giraldo G., and Ensoli B. The human immunodeficiency virus
type 1 Tat protein transactivates tumor necrosis factor beta gene expression through a TAR-like
structure. J. Virol. 68: 2677-2682, 1994.
21. Chang H.K., Gendelman R., Lisziewicz J., Gallo R.C., and Ensoli B. Block of HIV-1 infection
by a combination of antisense tat RNA and TAR decoys: A strategy for control of HIV-1. Gene
Therapy 1: 208-216, 1994.
22. Ensoli B., Gendelman R., Markham P., Fiorelli V., Colombini S., Raffeld M., Cafaro A., Chang
H.K., Brady J.N., and Gallo R.C. Synergy between basic fibroblast growth factor and HIV-1 Tat
protein in induction of Kaposi's sarcoma. Nature 371: 674-680, 1994.
23. Browning P.J., Sechler J.M.G., Kaplan M., Washington R.H., Gendelman R., Yarchoan R.,
Ensoli B., and Gallo R.C. Identification and culture of Kaposi's sarcoma-like spindle cells from
the peripheral blood of Human Immunodeficiency Virus-1-infected individuals and normal
controls. Blood 84: 2711-2720, 1994.
24. Ensoli B., Markham P., Kao V., Barillari G., Fiorelli V., Gendelman R., Raffeld M., Zon G.,
and Gallo R.C. Block of AIDS-Kaposi's sarcoma (KS) cell growth, angiogenesis, and lesion
2
formation in nude mice by antisense oligonucleotide targeting basic fibroblast growth factor. J.
Clin. Invest. 94: 1736-1746, 1994.
25. Chuah M.K.L., Vandendriessche T., Chang H.K., Ensoli B., and Morgan R.A. Inhibition of
Human Immunodeficiency Virus Type-1 by retroviral vectors expressing antisense-TAR. Hum.
Gene Ther. 5: 1467-1475, 1994.
26. Lisziewicz J., Sun D., Trapnell B., Thomson M., Chang H.K., Ensoli B., and Peng B. An
autoregulated dual-function antitat gene for human immunodeficiency virus type 1 gene
therapy. J. Virol. 69: 206-212, 1995.
27. Albini A., Barillari G., Benelli R., Gallo R.C., and Ensoli B. Angiogenic properties of human
immunodeficiency virus type 1 Tat protein. Proc. Natl. Acad. Sci. USA 92: 4838-4842, 1995.
28. Vandendriessche T., Chuah M.K.L., Chiang L., Chang H.K., Ensoli B., and Morgan R.A.
Inhibition of clinical human immunodeficiency virus (HIV) type 1 isolates in primary CD4+ T
lymphocytes by retroviral vectors expressing anti-HIV genes. J. Virol. 69: 4045-4052, 1995.
29. Chang H.K., Gallo R.C., and Ensoli B. Regulation of cellular gene expression and function by
the human immunodeficiency virus type 1 Tat protein. J. Biomed. Sci. 2:189-202, 1995.
30. Bohan Morris C., Gendelman R., Marrogi A.J., Lu M., Lockyer J.M., Alperin-Lea W., and
Ensoli B. Immunohistochemical detection of bcl-2 in AIDS-associated and classical Kaposi’s
sarcoma. Am. J. Pathol. 148: 1055-1063, 1996.
31. Brother M.B., Chang H.K., Lisziewicz J., Su D., Murty L.C., and Ensoli B. Block of Tatmediated transactivation of tumor necrosis factor ß gene expression by polymeric-TAR decoys.
Virology 222:252-256, 1996.
32. Lisziewicz J., Sun D., Gallo R.C., Ensoli B., and Lori F. Efficacy of antitat gene therapy in the
presence of high multiplicity infection of inflammatory cytokines. Human Gene Therapy
7:2209-2216, 1996.
33. Chang H.C., Samaniego F., Nair B.C., Buonaguro L., and Ensoli B. HIV-1 Tat protein exits
from cells via a leaderless secretory pathway and binds to extracellular matrix-associated
heparan sulfate proteoglycans through its basic region. AIDS 11:1421-1431, 1997.
34. Fiorelli V., Gendelman R., Sirianni M.C., Chang H.K., Colombini S., Markham P.D., Monini
P., Sonnabend J., Pintus A., Gallo R.C., and Ensoli B. γ-interferon produced by CD8+ T cells
infiltrating Kaposi’s sarcoma induces spindle cells with angiogenic phenotype and synergy with
Human Immunodeficiency Virus-1 Tat protein: an immune response to Human Herpes Virus-8
infection? Blood 91:956-967, 1998.
35. Ensoli B., and Stürzl M. Kaposi’s sarcoma: a result of the interplay among inflammatory
cytokines, angiogenic factors and viral agents. (Eds. M. Sporn and J.T. Vilcek) Cytokine and
Growth Factor Reviews 9:63-83, 1998.
36. Kelly G.D., Ensoli B., Gunthel C. J., and Offermann M.K. Purified Tat induces inflammatory
response genes in Kaposi’s sarcoma cells. AIDS 12:1753-1761, 1998.
3
37. Ensoli B. KS pathogenesis: role of citokynes, HIV-1 Tat protein and HHV-8 infection. EuroShaks, European Study on HIV associated Kaposi’s sarcoma (Workshop), Barcelona, June 4-5,
1998, pp. 51-66.
38. Fiorelli V., Barillari G., Toschi E., Sgadari C., Monini P., Stürzl M., and Ensoli B. IFN-γ
induces endothelial cells to proliferate and to invade the extracellular matrix in response to the
HIV-1 Tat protein: implications for AIDS-Kaposi’s sarcoma pathogenesis. J. Immunol.
162:1165-1170, 1999.
39.
Caselli E., Betti M., Grossi M.P., Balboni P.G., Rossi C., Boarini C., Cafaro A., BarbantiBrodano G., Ensoli B., and Caputo A. DNA Immunization with HIV-1 tat Mutated in the trans
Activation Domain Induces Humoral and Cellular Immune Responses Against Wild-Type Tat.
J. Immunol. 162:5631-5638, 1999.
40.
Cafaro A., Caputo A., Fracasso C., Maggiorella M.T., Goletti D., Baroncelli S., Pace M.,
Sernicola L., Koanga-Mogtomo M.L., Betti M., Borsetti A., Belli R., Åkerblom L., Corrias F.,
Buttò S., Heeney J., Verani P., Titti F., and Ensoli B. Control of SHIV89.6P-infection of
cynomolgus monkeys by HIV-1 Tat protein vaccine. Nat. Med. 5:643-650, 1999.
41.
Barillari G., Sgadari C., Palladino C., Gendelman R., Caputo A., Bohan Morris C., Nair B.C.,
Markham P., Nel A., Stürzl M., and Ensoli B. Inflammatory cytokines synergize with the HIV-1
Tat protein to promote angiogenesis and Kaposi’s sarcoma via induction of basic fibroblast
growth factor and αvβ3 integrin. J. Immunol. 163:1929-1935, 1999.
42.
Barillari G., Sgadari C., Fiorelli V., Samaniego F., Colombini S., Manzari V., Modesti A., Nair
B.C., Cafaro A., Stürzl M., and Ensoli B. The Tat protein of human immunodeficiency virus
type-1 promotes vascular cell growth and locomotion by engaging the α5β1 and αvβ3 integrins
by mobilizing sequestered basic fibroblast growth factor. Blood 94:663-672, 1999.
43.
Ensoli B., and Cafaro A. Control of viral replication and disease onset in cynomolgus monkeys
by HIV-1 TAT vaccine. J. Biol. Regul. and Homeost. Agents 14:22-26, 2000.
44.
Cafaro A., Caputo A., Maggiorella M.T., Baroncelli S., Fracasso C., Pace M., Borsetti A.,
Sernicola L., Negri D.R.M., Ten Haaft P., Betti M., Michelini Z., Macchia I., Fanales-Belasio
E., Belli R., Corrias F., Buttò S., Verani P., Titti F., and Ensoli B. SHIV89.6P pathogenicity in
cynomolgus monkeys and control of viral replication and disease onset by human
immunodeficiency virus type 1 Tat vaccine. J. Med. Primatol 29: 193-208, 2000.
45.
Ensoli B., and Cafaro A. Novel strategies toward the development of an effective vaccine to
prevent Human Immunodeficiency Virus infection or Acquired Immunodeficiency Virus. In:
AIDS Clinical Review 2000/2001, Volberding and Jacobson Eds., pp. 23-61.
46.
Cafaro A., Titti F., Fracasso C., Maggiorella M.T., Baroncelli S., Caputo A., Goletti D.,
Borsetti A., Pace M., Fanales-Belasio E., Ridolfi B., Negri D.R.M., Sernicola L., Belli R.,
Corrias F., Macchia I., Leone P., Michelini Z., ten Haaft P., Buttò S., Verani P., and Ensoli
B. Vaccination with DNA containing tat coding sequences and unmethylated CpG motifs
protects cynomolgus monkeys upon infection with simian/human immunodeficiency virus
(SHIV89.6P). Vaccine, 19:2862-2877, 2001.
47.
Bussolino F., Mitola S., Serini G., Barillari G., and Ensoli B. Interactions between
endothelial cells and HIV-1. Int. J. Biochem. Cell Biol., 33:371-390, 2001.
4
48.
Betti M., Voltan R., Marchisio M., Mantovani I., Boarini C., Nappi F., Ensoli B., and
Caputo A. Characterization of HIV-1 Tat proteins mutated in the transactivation domain for
prophylactic and therapeutic application. Vaccine, 19:3408-3419, 2001.
49.
Sirianni M.C., Libi F., Scaramuzzi D., Topino S., Campagna M., Colbacchi B., Novi A., De
Cristofaro M.R., Fiorelli V., Ensoli F., and Ensoli B. Modulation of the natural killer cell
activity of peripheral blood mononuclear cells by the HIV Tat protein. Proocedings of the 6th
European Conference on Experimental AIDS Research (ECEAR 2001), Edinburgh (Scotland),
June 23-26, 2001, pp.81-85.
50.
Toschi E., Barillari G., Sgadari C., Bacigalupo I., Cereseto A., Carlei D., Palladino C., Zietz
C., Leone P., Stürzl M., Buttò S., Cafaro A., Monini P., and Ensoli B. Activation of MatrixMetalloproteinase-2 and Membrane-Type-1-Matrix-Metalloproteinase in Endothelial Cells
and Induction of Vascular Permeability in vivo by the Human Immunodeficiency Virus-1
Tat protein and Basic Fibroblast Growth Factor. Mol. Biol. Cell, 12:2934-2946, 2001.
51.
Fanales-Belasio E., Moretti S., Nappi F., Barillari G., Micheletti F., Cafaro A., and Ensoli
B. Native HIV-1 Tat protein targets monocyte-derived dendritic cells and enhances their
maturation, function and antigen-specific T cell responses. J. Immunol., 168:197-206, 2002.
52.
Battistini A., Marsili G., Sgarbanti M., Ensoli B., and Hiscott J. Review: IRF Regulation of
HIV-1 Long Terminal Repeat Activity. J. Interferon Cytokine Res. 22:27-37, 2002.
53.
Ensoli B., and Cafaro A. HIV-1 Tat vaccines. Virus Res., 82(1-2):91-101, 2002.
54.
Barillari G., and Ensoli B. Angiogenic Effects of Extracellular Human Immunodeficiency
virus type 1 Tat Protein and its role in the pathogenesis of AIDS-associated Kaposi's
Sarcoma. Clin. Microbiol. Rev, 15:310-32, 2002.
55.
Caputo A., Betti M., Altavilla G., Bonaccorsi A., Boarini C., Marchisio M., Buttò S.,
Sparnacci K., Laus M., Tondelli L., and Ensoli B. Micellar-type complexes of tailor-made
synthetic block copolymers containing the HIV-1 tat DNA for vaccine application. Vaccine,
20:2303-2317, 2002.
56.
Sgarbanti M., Borsetti A., Moscufo N. , Bellocchi M.C., Ridolfi B., Nappi F., Marsili G.,
Marziali G., Coccia E.M., Ensoli B., and Battistini A. Modulation of HIV-1 Replication by
Interferon Regulatory Factors. J. Exp. Med., 195:1359-1370, 2002.
57.
Fanales-Belasio E., Cafaro A., Cara A., Negri D.R.M., Fiorelli V., Buttò S., Sonia Moretti,1
Moretti S., Maggiorella M.T., Baroncelli S., Michelini Z., Tripiciano A., Sernicola L.,
Scoglio A., Borsetti A., Ridolfi B., Bona R., ten Haaft P., Macchia I., Leone P., PavoneCossut M. R., Nappi F., Efthya Vardas,3 Mauro Magnani,4 Elena Laguardia,4 Antonella
Caputo,5 Vardas E., Magnani M., Laguardia E., Caputo A., Titti F., and Ensoli B. HIV-1
Tat-Based Vaccines: from Basic Science to Clinical Trials. DNA and Cell Biol., 21:599610, 2002.
58.
Caputo A., Gavioli R., Altavilla G., Brocca Cofano E., Boarini C., Betti M., Castaldello A.,
Lorenzini F., Micheletti F., Cafaro A., Sparnacci K., Laus M., Tondelli L., and Ensoli B.
Immunization with low doses of HIV-1 tat DNA delivered by novel cationic block
copolymers induces CTL responses against Tat. Vaccine, 21: 1103-1111, 2003.
5
59.
Dominici S., Laguardia M.E., Serafini G., Chiarantini L., Fortini C., Tripiciano A., BroccaCofano E., Scoglio A., Caputo A., Fiorelli V., Gavioli R., Cafaro A., Ensoli B., and
Magnani M. Red blood cell-mediated delivery of recombinant HIV-1 Tat protein in mice
induces anti-Tat neutralizing antibodies and CTL. Vaccine, 21:2082-2090, 2003.
60.
Borsutzky S., Fiorelli V., Ebensen T., Tripiciano A., Rharbaoui F., Scoglio A., Link C.,
Nappi F., Morr M., Buttò S., Cafaro A., Mühlradt P.F., Ensoli B., and Guzman CA.
Efficient mucosal delivery of the HIV-1 Tat protein using the synthetic lipopeptide MALP-2
as adjuvant. Eur. J. Immunol., 33:1548-1556, 2003.
61.
Marinaro M., Riccomi A., Rappuoli R., Pizza M., Fiorelli V., Tripiciano A., Cafaro A.,
Ensoli B., and De Magistris M.T. Mucosal delivery of the human immunodeficiency virus-1
Tat protein in mice elicits systemic neutralizing antibodies, cytotoxic T lymphocytes and
mucosal IgA. Vaccine, 21(25-26)-3503-4094, 2003.
62.
Buttò S., Fiorelli V., Tripiciano A., Ruiz-Alvarez M.J., Scoglio A., Ensoli F., Ciccozzi M.,
Collacchi B., Sabbatucci M., Cafaro A., Guzmán C.A., Borsetti A., Caputo A., Vardas E.,
Colvin M., Lukwyia M., Rezza G., Ensoli B., and the Tat Multicentric Study Group.
Sequence conservation and antibody cross-recognition of the clade B human
immunodeficiency virus (HIV) type 1 Tat Protein in HIV-1-Infected Italian, Ugandan and
South Africans. J. Infect. Dis., 188:1171-1180, 2003.
63.
Marsili G., Borsetti A., Sgarbanti M., Remoli A.L., Ridolfi B., Stellacci E., Ensoli B., and
Battistini A. On the role of interferon regulatory factors in HIV-1 replication. Ann. NY
Acad. Sci., 1010:29-42, 2003.
64.
Savarino A., Bensi T., Chiocchetti A., Bottarel F., Mesturini R., Ferrero E., Colosso L.,
Deraglio S., Ortolan E., Buttò S., Cafaro A., Katada T., Ensoli B., Malavasi F., and
Dianzani U. Human CD38 interferes with HIV-1 fusion through a sequence homologous to
the V3 loop of the viral envelope glycoprotein gp120. FASEB J., 17:461-463, 2003.
65.
Mooij P., Nieuwenhuis I.G., Knoop C.J., Doms R.W., Bogers W.M.J.M., Ten Haaft P.J.F.,
Niphuis H., Koornstra W., Bieler K., Koestler J., Morein B., Cafaro A., Ensoli B., Wagner
R., and Heeney J.L. Qualitative T-Helper Responses to Multiple Viral Antigens Correlate
with Vaccine-Induced Immunity to Simian/Human Immunodeficiency Virus Infection. J.
Virol., 78:3333-3342, 2004.
66.
Franzese O., Comandini A., Adamo R., Sgadari C., Ensoli B., Bonmassar E. HIV-Tat
down-regulates telomerase activity in the nucleus of human CD4+ T cells. Cell Death
Differ., 11:782-784, 2004.
67.
Cara A., Maggiorella M.T., Bona R., Sernicola L., Baroncelli S., Negri D.R.M., Leone P.,
Fagrouch Z., Heeney J., Titti F., Cafaro A., and Ensoli B. Circular viral DNA detection and
junction sequence analysis from PBMC of SHIV-infected cynomolgus monkeys with
undetectable virus plasma RNA. Virology, 324:531-9, 2004.
68.
Caputo A., Brocca-Cofano E., Castaldello A., Altavilla G., De Michele R. , Marchisio M.,
Gavioli R., Rolen U., Chiarantini L., Cerasi A., Dominici S., Magnani M., Cafaro A.,
Sparnacci K., Laus M., Tondelli L., and Ensoli B. Novel biocompatible anionic polymeric
microspheres for the delivery of the HIV-1 Tat protein for vaccine application. Vaccine,
22:2910-24, 2004.
6
69.
Maggiorella M.T., Baroncelli S., Michelini Z., Fanales-Belasio E., Moretti S., Sernicola L.,
Cara A., Negri D.R.M., Buttò S., Fiorelli V., Tripiciano A., Scoglio A., Caputo A., Borsetti
A., Ridolfi B., Bona R., ten Haaft P., Macchia I., Leone P., Pavone-Cossut M.R., Nappi F.,
Ciccozzi M., Heeney J., Titti F., Cafaro A., and Ensoli B. Long-term protection against
SHIV89.6P replication in HIV-1 Tat vaccinated cynomolgus monkeys. Vaccine, 22:32583269, 2004.
70.
Gavioli R., Gallerani E., Fortini C., Fabris M., Bottoni A., Canella A., Bonaccorsi A.,
Marastoni M., Micheletti F., Cafaro A., Rimessi P., Caputo A. and Ensoli B. HIV-1 Tat
protein modulates the generation of cytotoxic T cell epitopes by modifying proteasome
composition and enzymatic activity. J. Immunol., 173:3838-3843, 2004.
71. Caputo A., Gavioli R. and Ensoli B. Recent advances in the development of HIV-1 Tatbased vaccines. Curr. HIV Res., 2:357-376, 2004.
72.
Ferrantelli F., Cafaro A., and Ensoli B. Nonstructural HIV proteins as targets for
prophylactic or therapeutic vaccines. Curr. Opin. Biotech., 15:543-56, 2004.
73.
Ensoli B. AIDS Vaccine Integrated Project (AVIP). BIOforum Europe (01/2005), pp 38-40,
2005.
74.
Rezza G., Fiorelli V., Dorrucci M., Ciccozzi M., Tripiciano A. Scoglio A. 1, Collacchi B.,
Ruiz-Alvarez M., Giannetto C., Caputo A., Tomasoni L., Castelli F., Sciandra M., Sinicco
A., Ensoli F., Buttò S., and Ensoli B. The Presence of Anti-Tat Antibodies Is Predictive of
Long-Term Non-Progression to AIDS or Severe Immunodeficiency: Findings from a Cohort
of HIV Seroconverters. J. Infect. Dis., 191:1321-1324, 2005.
75.
Biassoni R., Fogli M., Cantoni C., Costa P., Conte R., Koopman G., Cafaro A., Ensoli B.,
Moretta A., Moretta L., De Maria A. Molecular and functional characterization of NKG2D,
NKp80, and NKG2C triggering NK cell receptors in rhesus and cynomolgus macaques:
monitoring of NK cell function during simian HIV infection. J. Immunol. 1:174:5695-5705,
2005.
76.
Zhao J., Voltan R., Peng B., Davis-Warren A., Kalyanaraman V.S., Alvord W.G., Aldrich
K., Bernasconi D., Buttò S., Cafaro A., Ensoli B., and Robert-Guroff M. Enhanced cellular
immunity to SIV Gag following co-administration of Adenoviruses encoding wild-type or
mutant HIV Tat and SIV Gag. Virology, 342:1-12, 2005.
77.
Ensoli B. Introduction: rational vaccine strategies against AIDS. Microbes Infect., 7:1385,
2005.
78.
Ensoli B. Rational vaccine strategies against AIDS: background and rationale. Microbes
Infect., 7:1445-1452, 2005.
79.
Ensoli B. Criteria for selection of HIV vaccine candidates-general principles. Microbes
Infect., 7:1433-1435, 2005.
80.
Ensoli B., Cafaro A., Caputo A., Fiorelli V., Ensoli F., Gavioli R., Ferrantelli F., Cara A.,
Titti F., and Magnani M. Vaccines based on the native HIV Tat protein and on the
combination of Tat and the structural HIV protein variant DeltaV2 Env. Microbes Infect.,
7
7:1392-1399, 2005.
81.
Borsutzky S., Ebensen T., Link C., Daniel Becker P., Fiorelli V., Cafaro A., Ensoli B., and
Guzmán C.A. Efficient systemic and mucosal responses against the HIV-1 Tat protein by
Prime/Boost vaccination using the lipopeptide MALP-2 as adjuvant. Vaccine, 24:20492056, 2006.
82.
Toschi E., Bacigalupo I., Strippoli R., Cereseto A., Falchi M., Chiozzini C., Nappi F.,
Sgadari C., Barillari G., Mainiero F., and Ensoli B. HIV-1 Tat regulates endothelial cell
cycle progression via activation of the Ras/ERK MAPK signaling pathway. Mol. Biol. Cell,
17:1985-1994, 2006.
83.
Remoli A.L., Marsili G., Pernotti E., Gallerani E., Ilari R., Nappi F., Cafaro A., Ensoli B.,
Gavioli R., and Battistini A. Intracellular HIV-1 tat protein represses constitutive LMP2
transcription increasing proteasome activity by interfering with the binding of IRF-1 to
STAT1. Biochem. J., 396:371-380, 2006.
84. Castaldello A., Brocca-Cofano E., Voltan R., Triulzi C., Altavilla G., Laus M., Sparnacci
K., Balestri M., Tondelli L., Fortini C., Gavioli R., Ensoli B., and Caputo A. DNA prime
and protein boost immunization with innovative polymeric cationic core-shell nanoparticles
elicits broad immune responses and strongly enhance cellular responses of HIV-1 tat DNA
vaccination. Vaccine, 24:5655-5669, 2006.
85.
Ensoli B., Fiorelli V., Longo O., Bellino S., Ensoli F., Tripiciano A., Scoglio A., Ruiz
M.,Collacchi B., Francavilla V., Lazzarin A., Tambussi G., Visintini R., Narciso P.,
D’Offizi G., Giulianelli M., Carta M., Di Carlo A., Palamara G., and Giuliani M.
Prophylactic and therapeutic Phase I trials with the active Tat protein vaccine: results of the
interim analysis. In: Antiviral Ther. 11 (Suppl. 2), International Medical Press, pag. 79,
2006 – from the: “AIDS Vaccine 2006 Conference”, Amsterdam, The Netherlands (August
29- September 1, 2006).
86.
Goletti D., Macchia I., Leone P., Pace M., Sernicola L., Pavone-Cossut M.R., Maggiorella
M.T., Cafaro A., Ensoli B., and Titti F. Innate anti-viral immunità is associated with the
protection elicited by the Simian Immunodeficiency Virus (SIV) live attenuated virus
vaccine in cynomolgus monkeys. Med. Sci. Monit., 12:BR330-340, 2006.
87.
Ferrantelli F., Buttò S., Cafaro A., Wahren B., and Ensoli B. Building Collaborative
Networks for HIV/AIDS Vaccine Development: the AVIP experience. Springer Semin.
Immunopathol., 28:289-301, 2006.
88.
Ensoli B., Fiorelli V., Ensoli F., Cafaro A., Titti F., Buttò S., Monini P., Magnani M.,
Caputo A., and Garaci E. Candidate HIV-1 Tat vaccine development: from basic science to
clinical trials. AIDS, 20:2245–2261, 2006.
89.
Bozac A., Berto E., Vasquez F., Grandi P., Caputo A., Manservigi R., Ensoli B., and
Marconi P. Expression of human immunodeficiency virus type 1 tat from a replicationdeficient herpes simplex type 1 vector induces antigen-specific T cell responses. Vaccine,
24:7148-7158, 2006.
90.
Demberg T., Florese R.H., Gomez-Roman V.R., Larsen K., Van Rompay K.K., Marthas
M.L., Venzon D., Kalyanaraman V., Pal R., Barnett S.W., Cafaro A., Ensoli B., and Robert8
Guroff M. Non-neutralizing antibodies and vaccine-induced protection. Retrovirology,
3(Suppl 1):S26, 2006.
91.
Titti F., Cafaro A., Ferrantelli F., Tripiciano A., Moretti S., Caputo A., Gavioli R., Ensoli F.,
Robert-Guroff M., Barnett S., and Ensoli B. Problems and emerging approaches in
HIV/AIDS vaccine development. Exp. Opin. Emerg. Drugs, 12:23-48, 2007.
92.
Demberg T., Florese R.H., Heath M.J., Larsen K., Kalisz I., Kalyanaraman V.S., Lee E.M.,
Pal R., Venzon D., Grant R., Patterson L.J., Korioth-Schmitz B., Buzby A., Dombagoda D.,
Montefiori D.C., Letvin N.L., Cafaro A., Ensoli B., and Robert-Guroff M. A replicationcompetent Ad-HIVtat and –HIVenv priming/1 Tat and Envelope protein boosting regimen
elicits enhanced protective efficacy against SHIV89.6P challenge in rhesus macaques. J.
Virol., 81:3414-3427, 2007.
93. Bråve A., Hinkula J., Cafaro A., Eriksson L.E., Srivastava I.K., Magnani M., Ensoli B.,
Barnett S.W., Wahren B., Rollman E. Candidate HIV-1 gp140ΔV2, Gag and Tat vaccines
protect against experimental HIV-1/MuLV challenge. Vaccine, 25:6882-6890, 2007.
94. Gavioli R., Cellini S., Castaldello A., Voltan R., Gallerani E., Gagliardoni F., Fortini C.,
Brocca-Cofano E.., Triulzi C., Cafaro A., Srivastava I., Barnett S., Caputo A., and Ensoli B.
The Tat protein broadens T cell responses directed to the HIV-1 antigens Gag and Env:
Implications for the design of new vaccination strategies against AIDS. Vaccine, 26:727737, 2008.
95. Caputo A., Brocca-Cofano E., Castaldello A., Voltan R., Gavioli R., Srivastava I.K., Barnett
S.W., Cafaro A., and Ensoli B. Characterization of immune responses elicited in mice by
intranasal co-immunization with HIV-1 Tat, gp140 ΔV2Env and/or SIV Gag proteins and
the nontoxicogenic heat-labile Escherichia coli enterotoxin. Vaccine, 26:1214-1227, 2008.
96. Ridolfi B., Genovese D., Argentini C., Maggiorella M.T., Sernicola L., Buttò S., Titti F.,
Borsetti A., and Ensoli B. Tat protein vaccination of cynomolgus macaques influences
SHIV-89.6Pcy243 epitope variability. Virus Genes, 36:105-115, 2008.
97. Borsetti A., Baroncelli S., Maggiorella M.T., Bellino S., Moretti S., Sernicola L., Belli R.,
Ridolfi B., Farcomeni S., Negri D.R.M., Cafaro A., Ensoli B., and Titti F. Viral outcome of
simian-human immunodeficiency virus SHIV-89.6P adapted to cynomolgus monkeys. Arch.
Virol., 153:463-472, 2008.
98. Sgarbanti M., Remoli A.L., Marsili G., Ridolfi B., Borsetti A., Perrotti E., Orsetti R., Ilari R.,
Sernicola R., Stellacci E., Ensoli B., Battistini A. IRF-1 is required for full NF-κb
transcriptional activity at the HIV-1 LTR enhancer. J. Virol., 82:3632-3641, 2008.
9
99. Florese R.H., Wiseman R.W., Venzon D., Karl J.A., Demberg T., Larsen K., Flanary L.,
Kalyanaraman V.S., Pal R., Titti F., Patterson L.J., Heath M.J., O'Connor D.H., Cafaro A.,
Ensoli B., and Robert-Guroff M. Comparative study of Tat vaccine regimens in Mauritian
cynomolgus and Indian rhesus macaques: influence of Maritian MHC haplotypes on
susceptibility/resistance to SHIV896P infection. Vaccine, 26:3312-3321, 2008.
100. Ensoli B., Fiorelli V., Ensoli F., Lazzarin A., Visintini R., Narciso P., Di Carlo A., Monini
P. Magnani M., and Garaci E. The therapeutic phase I trial of the recombinant native HIV-1
Tat protein. AIDS, 22:2207-2209, 2008.
101. Fanales-Belasio E., Moretti S., Fiorelli V., Tripiciano A, Pavone-Cossut M.R., Scoglio A.,
Collacchi B., Nappi F., Macchia I., Bellino S., Francavilla V., Caputo A., Barillari G.,
Magnani M., Laguardia M.E., Cafaro A., Titti F., Monini P., Ensoli F., and Ensoli B. HIV-1
Tat addresses dendritic cells to induce a predominant Th1-type adaptive immune response
which appears prevalent in the asymptomatic stage of infection. J. Immunol., 182:28882897, 2009.
102. Florese R.H., Demberg T., Xiao P., Kuller L., Larsen K., Summers E.L., Venzon D., Cafaro
A., Ensoli B., and Robert-Guroff M. Contribution of non-neutralizing vaccine-elicited
antibody activities to improved protective efficacy in rhesus macaques immunized with
Tat/Env compared to multigenic vaccines. J. Immunol., 182:3718-27, 2009.
103. Borsetti A., Baroncelli S., Maggiorella M.T., Moretti S., Fanales Belasio E., Sernicola L.,
Tripiciano A., Macchia I., Michelini Z., Belli R., Farcomeni S., Pavone-Cossut M.R.,
Negri D., Caputo A., Bellino S., Butto' S., Titti F., Cafaro A., and Ensoli B. Containment of
infection in Tat vaccinated monkeys after rechallenge with a higher dose of SHIV89.6Pcy243.
Viral Immunol., 22:117-24, 2009.
104. Longo O., Tripiciano A., Fiorelli V., Bellino S., Scoglio A., Collacchi B., Ruiz Alvarez M.J.,
Francavilla V., Arancio A., Paniccia G., Lazzarin A., Tambussi G., Tassan Din C., Visintini
R., Narciso P., Antinori A., D’Offizi G., Giulianelli M., Carta M., Di Carlo A., Palamara G.,
Giuliani M., Laguardia M.E., Monini P., Magnani M., Ensoli F., and Ensoli B. Phase I
therapeutic trial of the HIV-1 Tat protein and long term follow-up. Vaccine, 27:3306-3312,
2009.
105. Caputo A., Castaldello A., Brocca-Cofano E., Voltan R., Bortolazzi F., Altavilla G.,
Sparnacci K., Laus M., Tondelli L., Gavioli R., and Ensoli B. Induction of humoral and
enhanced cellular immune responses by novel core-shell nanosphere- and microspherebased vaccine formulations following systemic and mucosal administration. Vaccine,
27:3605-3615, 2009.
106. Voltan R., Castaldello A., Brocca-Cofano E., De Michele R., Triulzi C., Altavilla G.,
Tondelli L., Laus M., Reali E., Gavioli R., Ensoli B., Caputo A. Priming with a very low
dose of DNA complete with cationic block copolymers follone by protein boosts elicits
broad and long-lasting antigen-specific humoral and cellular responses in mice. Vaccine,
27:4498–4507, 2009.
107. Cafaro A., Macchia I., Maggiorella M.T., Titti F., and Ensoli B. Innovative approaches to
develop prophylactic and therapeutic vaccines against HIV/AIDS. In: Pharmaceutical
10
Biotechnology (Guzman C.A. and Fuerstein G. Eds.), Chapter No. 14, pp. 189-242,
Publisher: Landes Bioscience/Eurekah, USA, 2009.
108. Caputo A., Gavioli R., Bellino S., Longo O., Tripiciano A., Francavilla V., Sgadari C.,
Paniccia G., Titti F. Cafaro A., Ferrantelli F., Monini P., Ensoli F., and Ensoli B. HIV-1 Tatbased vaccines: an overview and perspectives in the field of HIV/AIDS vaccine
development. Int. Reviews Immunol., 28:285–334, 2009.
109. Nappi F., Chiozzini C., Bordignon V., Borsetti A., Bellino S., Cippitelli M., Barillari G.,
Caputo A., Tyagi M., Giacca M., and Ensoli B. Immobilized HIV-1 Tat protein promotes
gene transfer via a transactivation-independent mechanism which require binding of Tat to
viral particles. J. Gene Med., 11:955–965, 2009.
110. Ensoli B., Fiorelli V., Ensoli F., Lazzarin A., Visintini R., Narciso P., Di Carlo A.,
Tripiciano A., Longo O., Bellino S., Francavilla V., Paniccia G., Arancio A., Scoglio A.,
Collacchi B., Ruiz Alvarez M.J., Tambussi G., Tassan Din C., Palamara G., Latini A.,
Antinori A., D’Offizi G., Giuliani M., Giulianelli M., Carta M., Monini P., Magnani M., and
Garaci E. The preventive phase I trial with the HIV-1 Tat based vaccine. Vaccine, 28:371–
378, 2009.
111. Bellino S., Francavilla V., Tripiciano A., Paniccia G., Arancio A., Fiorelli V., Scoglio A.,
Collacchi B., Campagna M., Lazzarin A., Tambussi G., Tassan Din C., Visintini R.,
Narciso P., Antinori A., D'Offizi G., Giulianelli M., Carta M., Di Carlo A., Palamara G.,
Giuliani M., Laguardia M.E., Monini P., Magnani M., Ensoli F., and Ensoli B. Parallel
conduction of the phase I preventive and therapeutic trials based on the Tat vaccine
candidate. Recent Rev. Clin. Trials, 4:195-204, 2009.
112. Bernasconi D., Tavoschi L., Regine V., Raimondo M., Gama D., Sulgencio L., Almaviva
M., Galli C., Ensoli B., Suligoi B., Sukati H. and Buttò S. Indentification of recent HIV
infections and of factors associated with virus acquisition among pregnant women in 2004
and 2006 in Swaziland. Journal of Clinical Virology, 48: 180-183, 2010.
113. Cafaro A., Bellino S., Titti F., Maggiorella M.T., Sernicola L., Wiseman W. R., Venson D.,
Karl A. J., O’Connor D., Monini P., Robert-Guroff M., Ensoli B. Impact of Viral Dose and
Major Histocompatibility Complex Class IB Haplotype on Viral Outcome in Tat-vaccinated
Mauritian Cynomolgus Monkeys upon Challenge with SHIV89.6P J Virol., 84: :8953-8,
2010.
114. Pierleoni R, Menotta M., Antonelli A, Sfara C., Serafini G., Dominici S., Laguardia M.E.,
Salis A., Damonte G., Banci L., Porcu M., Monini P., Ensoli B., Magnani M. Effect of the
redox state on HIV-1 tat protein multimerization and cell internalization and trafficking. Mol
Cell Biochem. 345:105-18, 2010.
115. Ensoli B, Bellino S, Tripiciano A, Longo O, Francavilla V, Marcotullio S, Cafaro A, Picconi
O, Paniccia G, Scoglio A, Arancio A, Ariola C, Ruiz Alvarez MJ, Campagna M, Scaramuzzi
D, Iori C, Esposito R, Mussini C, Ghinelli F, Sighinolfi L, Palamara G, Latini A, Angarano
G, Ladisa N, Soscia F, Mercurio V S, Lazzarin A, Tambussi G, Visintini R, Mazzotta F, Di
Pietro M, Galli M, Rusconi S, Carosi G, Torti C, Di Perri G, Bonora S, Ensoli F, Garaci E.
Therapeutic Immunization with HIV-1 Tat Reduces Immune Activation and Loss of
Regulatory T-Cells and Improves Immune Function in Subjects on HAART. PLoS ONE,
11
5:e13540, 2010.
116. Luzi A.M., Gallo P., Colucci A., Marcotullio S., Bellino S., Longo O., Ensoli B.
Communication, recruitment and enrolment in the preventative and therapeutic phase I
clinical trial against HIV/AIDS based on the recombinant HIV-1 Tat protein. Aids Care, 9:
1-8, 2011.
117. Ferrantelli F., Maggiorella M.T., Schiavoni I., Sernicola L., Olivieri E., Farcomeni S.,
Pavone-Cossut M.R., Moretti S., Belli R., Collacchi B., Srivastava I.K., Titti F., Cafaro A.,
Barnett S.W., Ensoli B. A combination HIV vaccine based on Tat and Env proteins was
immunogenic and protected macaques from mucosal SHIV challenge in a pilot study.
Vaccine, 29: 2918–2932, 2011.
118. Sgadari C, Barillari G, Palladino C, Bellino S, Taddeo B, Toschi E, Ensoli B. Fibroblast
growth factor-2 and the HIV-1 Tat protein synergize in promoting Bcl-2 expression and
preventing endothelial cell apoptosis: implications for the pathogenesis of AIDS-associated
Kaposi’s sarcoma. Int J Vasc Med. 2011:452729. 2011
119. Fraternale A, Paoletti MF, Dominici S, Buondelmonte C, Caputo A, Castaldello A,
Tripiciano A, Cafaro A, Palamara AT, Sgarbanti R, Garaci E, Ensoli B, Magnani M.
Modulation of Th1/Th2 immune responses to HIV-1 Tat by new pro-GSH molecole.
Vaccine. 29:6823-6829. 2011.
120. Monini P, Cafaro A, Srivastava IK, Moretti S, Sharma VA, Andreini C, Chiozzini C,
Ferrantelli F, Cossut MR, Tripiciano A, Nappi F, Longo O, Bellino S, Picconi O, FanalesBelasio E, Borsetti A, Toschi E, Schiavoni I, Bacigalupo I, Kan E, Sernicola L, Maggiorella
MT, Montin K, Porcu M, Leone P, Leone P, Collacchi B, Palladino C, Ridolfi B, Falchi M,
Macchia I, Ulmer JB, Buttò S, Sgadari C, Magnani M, Federico MP, Titti F, Banci L,
Dallocchio F, Rappuoli R, Ensoli F, Barnett SW, Garaci E, Ensoli B. HIV-1 Tat Promotes
Integrin-Mediated HIV Transmission to Dendritic Cells by Binding Env Spikes and
Competes Neutralization by Anti-HIV Antibodies. PLoS ONE. 7:e48781. 2012
12