Uveiti
associate a malattie reumatiche
Adriana Bonora
Clinica Oculistica
Az. Ospedaliera Universitaria Integrata
Verona
Quali sono le malattie reumatiche che
interessano l’occhio
·
·
·
·
·
·
·
Artrite reumatoide
Sindrome di SjÖgren
Malattia di Behçet
Artrite idiopatica giovanile
Artriti reattive
Spondilite anchilosante
Lupus eritematoso sistemico
· Sclerodermia
· Polidermatomiosite
· Granulomatosi di
Wegener
· Arterite a cellule giganti
· Poliarterite nodosa
· Granulomatosi allergica
· Arterite di Takayasu
Perché viene colpito l’occhio
• L'occhio, come altri organi, può essere colpito da
processi autoimmuni ed autoinfiammatori per
alterazione dei meccanismi immunitari (innati e
adattativi)
Quali sono le manifestazioni più
comuni in corso di malattia reumatica
Ogni malattia si può manifestare tipicamente con un interessamento
oculare diverso.
• Occhio secco (Sindrome di SjÖgren, Artrite reumatoide, Lupus
eritematoso sistemico, Sclerodermia)
• Uveite anteriore acuta, cronica, recidivante (Spondilite
anchilosante, Artrite idiopatica giovanile, M. di Beçhet)
• Uveite posteriore (M. di Beçhet)
• Episclerite (Artrite reumatoide, Poliarterite nodosa, Lupus
eritematoso sistemico, M. di Beçhet)
• Sclerite (Artrite reumatoide, Arterite di Wegener)
***********
• Cheratiti periferiche ulcerative (Artrite reumatoide, Arterite di
Wegener, Poliarterite nodosa)
• Vasculiti retiniche (Lupus eritematoso sistemico)
• Otticopatie anteriori e posteriori (Arterite a cellule giganti)
La comparsa di una patologia oculare può
essere:
· il primo segno di una manifestazione
reumatica sistemica
· il segno di una riattivazione della patologia
· può indicare la gravità della malattia reumatica
· può essere bersaglio degli effetti collaterali dei
farmaci usati per la malattia reumatica
Quale è il ruolo dell’oculista
· Gestire le manifestazioni
oculari
· Indirizzare alla diagnosi
· Collaborare con il
reumatologo
· Controllare gli effetti
collaterali dei farmaci
Uveiti
Uveiti
• anamnesi oculare
• anamnesi generale
• esame obiettivo oculare
- localizzazione anatomica
- caratteristiche tipiche
- tipo di infiammazione
• esami selettivi
CLASSIFICAZIONE DELLE UVEITI DEL SUN* WORKING GROUP
Sito primario infiammazione
Manifestazioni
Camera anteriore
Iridociclite
Ciclite anteriore
Vitreo
Pars planite
Ciclite posteriore
Ialite
Uveiti
posteriori
Retina o coroide
Coroidite
(focale, multifocale o diffusa)
Corioretinite
Retinocoroidite
Retinite
Neuroretinite
Panuveiti
Camera anteriore, vitreo,
retina, coroide
Uveiti
anteriori
Uveiti
intermedie
*SUN = Standardization of uveitis nomenclature
Esame obiettivo
Segni caratteristici
possono orientarci
nella diagnosi
in pochi minuti
Uveiti anteriori granulomatose
• Idiopatica
• Sarcoidosi
• Tubercolosi
• Sifilide
• Sclerosi multipla
• Malattia di Lyme
Uveiti anteriori non granulomatose
• Idiopatica
• HLA-B27 correlata
• Ciclite eterocromica di
Fuchs
• Artrite idiopatica
giovanile
• Malattia di Behçet
• Uveite associata a
sclerite
• TINU (nefrite tubulointerstiziale associata ad
uveite)
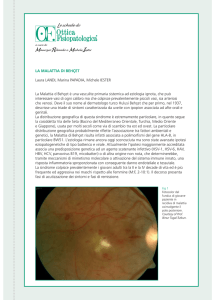
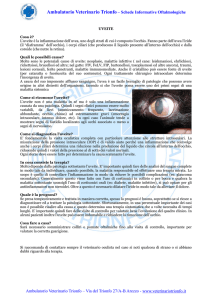
Artrite idiopatica giovanile
Artrite idiopatica giovanile
•
•
•
•
•
•
•
•
la più comune causa di uveite nei bambini
uveite presente nel 20-30% dei casi di AIG
3: 1
iridociclite asintomatica
sinechie
cheratopatia a bandelletta
cataratta
glaucoma
Artrite idiopatica giovanile
AIG
Artrite idiopatica giovanile
Intervallo uveite-AIG
Severità
Gestione AIG
•
•
•
•
•
controllo oculistico periodico
tropicamide
steroidi topici (cell in CA)
controllo TOO (successo chirurgia filtrante < 50%)
chirurgia della cataratta (!!!)
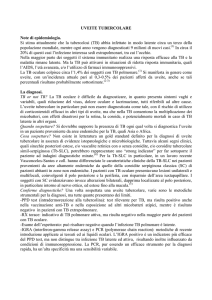
Uveite HLA B27 correlata
Sindromi HLA B27 correlate
• uveite anteriore acuta
• spondilite anchilosante
• artrite reattiva a infezioni genitourinarie o
gastointestinali (sr. di Reiter)
• malattie infiammatorie croniche dell’intestino
(RCU e m. di Crohn)
• artrite psoriasica
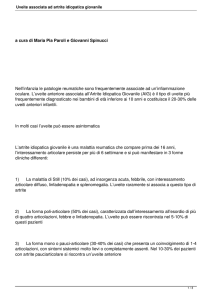
Uveite HLA B27+
• uveite anteriore acuta monolaterale
• non granulomatosa
• triade:
iperemia pericheratica
dolore
fotofobia
• fini precipitati endoteliali
• intensa risposta cellulare
• fibrina in CA
• I° attacco < 40 aa
• recidivante
• spesso associata con spondiloartropatie sieronegative
Uveite HLA B27+
Sacroileite
Progressione della spondilite
anchilosante
Trattamento
•
•
•
STEROIDI: topici, perioculari, orali, intravitreali
MIDRIATICI
TERAPIA IMMUNOSOPPRESSIVA:
• casi refrattari
• effetti avversi degli steroidi
• corticodipendenza
• rischio di danni visivi permanenti
– azatioprina, methotrexate, ciclosporina, ciclofosfamide, clorambucile
– agenti biologici antiTNF:
• etanercept
• infliximab
• adalimumab
(Enbrel)
(Remicade)
(Humira)
– interferon alpha
• IFNα-2a
– sulfasalazina (artriti reattive)
•
CONSULENZA REUMATOLOGICA
Br J Ophthalmol. 2010 Oct 22.
Distress, depression and coping in HLA-B27-associated anterior uveitis with
focus on gender differences.
Maca SM, Schiesser AW, Sobala A, Gruber K, Pakesch G, Prause C, BarisaniAsenbauer T.
Medical University Vienna, Vienna, Austria.
Patients with B27-AU patients exhibited significant
psychopathology concerning depression and disease coping.
Distress and life events were subjectively suspected to be a
trigger. By imparting knowledge to the patients on probable
development of depressive moods and the role of stress/life
events as trigger for relapses, as well as offering behaviour
therapy to optimise coping, may help patients to cope better
with B27-AU.
Malattia di Behçet
Hulûsi Behçet (1889–1948)
• età 30 anni
• bacino Mediterraneo - Oriente
• cause multifattoriali
– genetiche (HLA B51)
– infettive (Streptococcus sanguis, HSV)
– immunologiche
• decorso cronico recidivante
• diagnosi clinica:
Criteria for diagnosis of Behçet's disease.
International Study Group for Behçet's Disease.
Lancet. 1990 May 5;335(8697):1078-80
CRITERI MAGGIORI
• afte orali (99.3%)
• uveite
80% bilaterale, 20% monolaterale
– anteriore (60%)
– posteriore (75%)
– panuveite (90%)
• lesioni cutanee: pseudofollicolite,
eritema nodoso, lesioni
papulopustolose, noduli acneiformi
• afte genitali (60%)
• pathergy test positivo
CRITERI MINORI
•
•
•
•
•
artrite
ulcere ileocecali
epididimite
lesioni vascolari
sintomi neurologici
Laboratorio
• HLA B51
• anemia e leucocitosi
• aumento VES e Proteina
C reattiva
• aumento
alfa2globuline, IgA
• immunocomplessi
circolanti
• assenza FR e ANA
Joint Bone Spine. 2010 Jul;77(4):330-4. Epub 2010 May 8.
A study on thrombophilic factors in Italian Behcet's patients.
Caramaschi P, Poli G, Bonora A, Volpe A, Tinazzi I, Pieropan S, Bambara LM, Biasi D.
BACKGROUND: Behcet's disease (BD) may complicate with arterial and venous thrombosis. The purpose of this
work is to evaluate in an Italian group of BD patients with thrombotic events a large panel of inherited and
acquired thrombophilic factors.
METHODS: Thirty BD patients, of which nine with previously arterial or venous thrombosis and 21 without,
underwent the following investigations: plasma antithrombin activity, protein C activity,
free protein S level, sensitivity to APC, total plasma homocysteine concentration,
serum folate level, determination of anti-phospholipid antibodies, serum Lp(a)
levels, tests for gene polymorphisms of factor V Leiden, prothrombin and
methylenetetrahydrofolate reductase genes. Tests for the gene polymorphisms were also
performed in a group of healthy control subjects.
RESULTS: All the six patients with arterial or deep venous thrombosis showed thrombophilic conditions such as
protein C or protein S deficiency (one case each), hyperhomocysteinemia (two cases), positivity of antiphospholipid antibodies associated with APC resistance or hyperhomocysteinemia (one case each). Among
three subjects with superficial thrombophlebitis only one showed a mild hyperhomocysteinemia. No
differences were found between BD patients and control subjects concerning polymorphisms of the genes
considered. Among BD patients the Factor V H1299R mutation showed a weak association with venous
thrombosis (P=0.048).
CONCLUSION: In BD patients different concomitant significant thrombophilic risk
factors may contribute to the development of thrombotic events. Patients
affected by vasculo-Behcet should be evaluated for the presence of coexisting
major thrombophilic conditions.
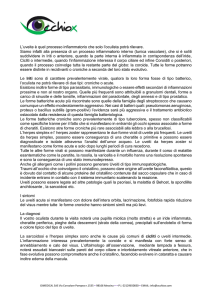
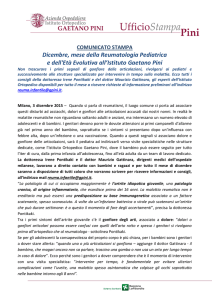
Manifestazioni oculari
• sono precoci
• il coinvolgimento oculare è
il più grave e il più temuto
→ cecità
• interessa il 60-80% dei pz
con M. di Behçet
• uveite posteriore con
vasculite occlusiva
venosa e arteriosa
(più raramente u. anteriore,
sclerite, neurite ottica)
Ipopion
•
•
Ophthalmology. 2010 Feb;117(2):366-72.
Hypopyon in patients with uveitis.
•
Zaidi AA, Ying GS, Daniel E, Gangaputra S, Rosenbaum JT, Suhler EB, Thorne JE,
Foster CS, Jabs DA, Levy-Clarke GA, Nussenblatt RB, Kempen JH; Systemic
Immunosuppressive Therapy for Eye Diseases Cohort Study.
•
•
4911 pazienti
CONCLUSIONS: Hypopyon is an uncommon occurrence in patients
with uveitis. Risk factors included Behçet's disease, HLA-B27
positivity, and spondyloarthropathy. Intermediate uveitis cases (+/anterior uveitis) had a lower risk of hypopyon. On average, posthypopyon eyes were no more likely than other eyes with uveitis to
develop structural ocular complications or lose visual acuity.
Conseguenze
•
•
•
•
•
manicotti vascolari
cicatrici corioretiniche
atrofia retinica
atrofia ottica
neovascolarizzazione
retinica
• glaucoma neovascolare
→CECITA’
EULAR RECOMMENDATIONS FOR THE
MANAGEMENT OF BEHÇET’S DISEASE
Ann Rheum Dis, 2008
1. Any patient with BD and inflammatory eye disease affecting
the posterior segment should be on a treatment regime,
which includes azathioprine and systemic corticosteroids
2. If the patient has severe eye disease defined as >2 lines of
drop in visual acuity on a 10/10 scale and/or retinal disease
(retinal vasculitis or macular involvement), it is recommended
that either cyclosporine A or infliximab be used in
combination with azathioprine and corticosteroids;
alternatively interferon-alpha with or without
corticosteroids could be used instead
Terapia
SOMMINISTRAZIONE TOPICA CS
desametazone 2%
• uveiti anteriori
SOMMINISTRAZIONE PERIOCULARE CS
betametasone disodio fosfato
metilprednisolone acetato
• u. anteriori non controllate
dalla terapia topica
• u. intermedie
• u. posteriori acute
• u. diffuse
SOMMINISTRAZIONE SISTEMICA CS
prednisone
metilprednisolone
• u. anteriori, intermedie, posteriori non
sufficientemente controllate dalla terapia
topica e/o perioculare
• u. bilaterali posteriori e diffuse
• u. associate a malattie sistemiche
SOMMINISTRAZIONE ENDOBULBARE CS
triamcinolone
• uveiti gravi in cui non è
praticabile la terapia
corticosteroidea per via
sistemica
• edema maculare
dexamethasone intravitreal implant
0.7 mg
Ocul Immunol Inflamm. 2010 Oct 31.
Clinical Review: Update on Treatment of Inflammatory Macular Edema.
Ossewaarde-van Norel A, Rothova A.
Department of Ophthalmology, University Medical Center Utrecht, Utrecht, The
Netherlands.
The aim of this review is to summarize the recent developments in the treatment of
inflammatory macular edema (ME). Inflammatory ME represents a major cause of
visual loss in uveitis and its adequate management is crucial for the maintenance
of useful vision in patients with uveitis. Recent studies favor early treatment of
inflammatory ME, even in patients with full visual acuity. After recapitulating the
standard treatment modalities for inflammatory ME the authors address novel
corticosteroid implants. They review the literature on the efficacy of anti-VEGF
agents for inflammatory ME and point out their beneficial, but transient effects.
Further, they present recent data on the value of systemic biologics in uveitic ME
and evaluate the effectiveness of vitrectomy. Finally, they propose an algorithm for
the treatment of inflammatory ME and point out that the individual risk-benefit
ratio, especially with systemic immunosuppressive therapy, should always be
considered.
IMMUNOSOPPRESSORI
INDICAZIONI
ASSOLUTE:
INDICAZIONI
RELATIVE:
• M. di Behçet
• uveite simpatica
steroido-resistente
• uveiti bilaterali,
non infettive,
corticoresistenti,
con prognosi visiva
infausta
ANTIMETABOLITI e AGENTI ALCHILANTI
Utilizzati in associazione con steroidi e/o
ciclosporina per ridurne i singoli dosaggi.
• EFFETTI COLLATERALI:
leucopenia, trombocitopenia,
epato-nefrotossicità, effetti carcinogenetici,
effetti teratogeni, azoospermia irreversibile.
ANTIMETABOLITI
• AZATIOPRINA
1-2.5 mg/kg/die x os
• METHOTREXATE
7.5-15 mg/sett x os o IM
AGENTI ALCHILANTI
• CLORAMBUCILE
• CICLOFOSFAMIDE
(Leukeran 2 mg)
(Endoxan 50 mg)
6-12/mg/die
2 mg/kg/die
CICLOSPORINA A
•
•
•
•
5 mg/kg/die in due somministrazioni
riduzione graduale fino a 2 mg/kg/die
durata terapia?
effetto rebound
CICLOSPORINA A
EFFETTI COLLATERALI:
•
•
•
•
•
•
ipertensione arteriosa
anemia
iperuricemia
aumento VES
aumento transaminasi
nefrotossicità
Farmaci Biologici nel
trattamento delle Uveiti
• agenti biologici antiTNF:
• etanercept
• infliximab
• adalimumab
• interferon alpha
• IFNα-2a
(Enbrel)
(Remicade)
(Humira)
Agenti biologici antiTNF:
• uveite associata alle SpA
• uveite associata alla artrite idiopatica
giovanile
• uveite posteriore
– m. di Behçet
– panuveite
– vasculite
Interferon alpha
• M. di Behçet
• VKH